Downloaded 335 times
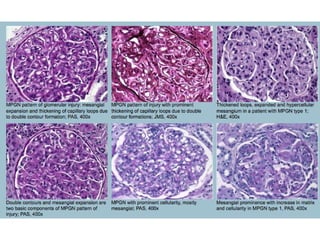
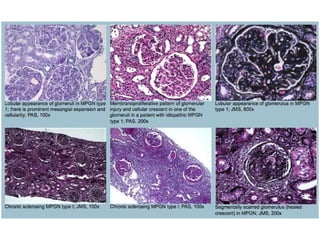
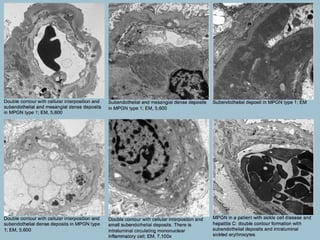
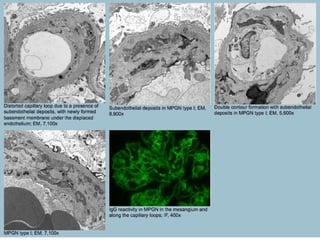
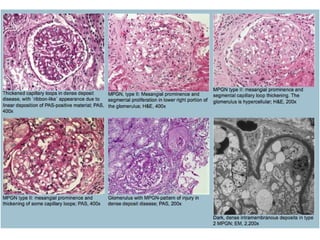
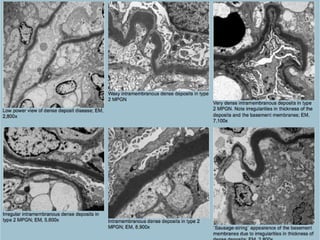
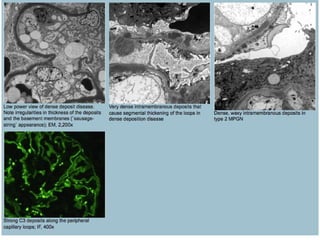
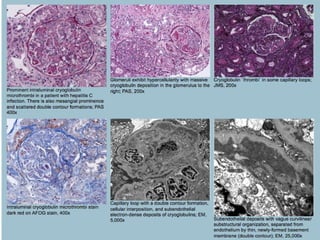
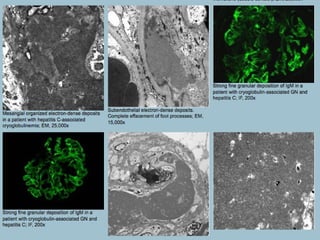
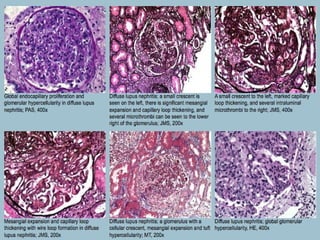
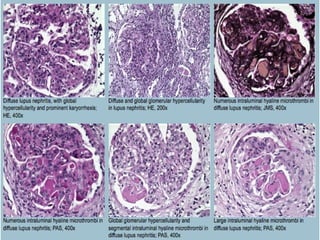
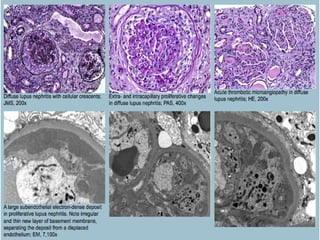
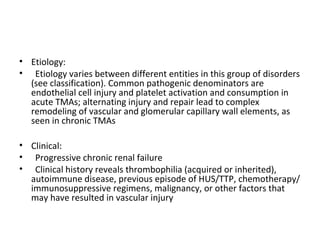
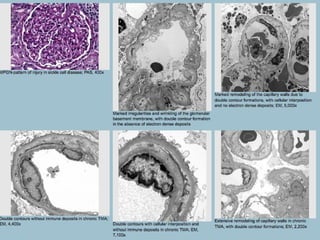
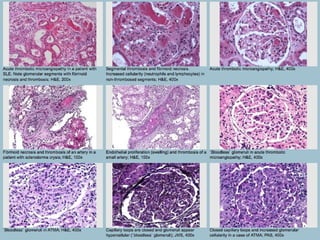

This document discusses several types of glomerular diseases that present with a membranoproliferative pattern of injury on histology, including membranoproliferative glomerulonephritis (MPGN) types I, II, and III, cryoglobulin-associated glomerulonephritis, lupus nephritis class IV, and thrombotic microangiopathies (both acute and chronic). It provides details on the etiology, clinical features, histopathology, immunofluorescence, and electron microscopy findings of each condition.


























































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









