Download as POT, PPTX

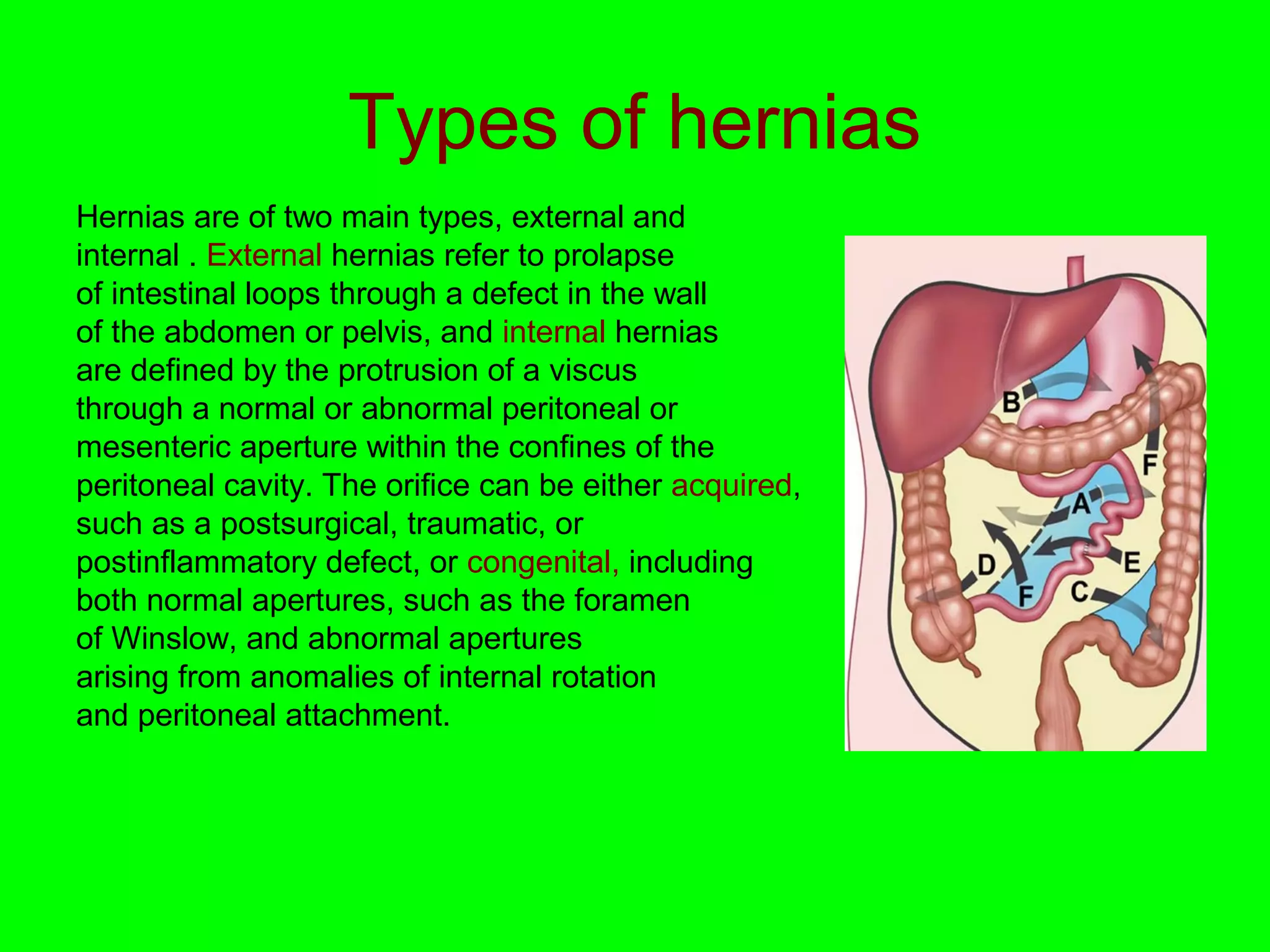
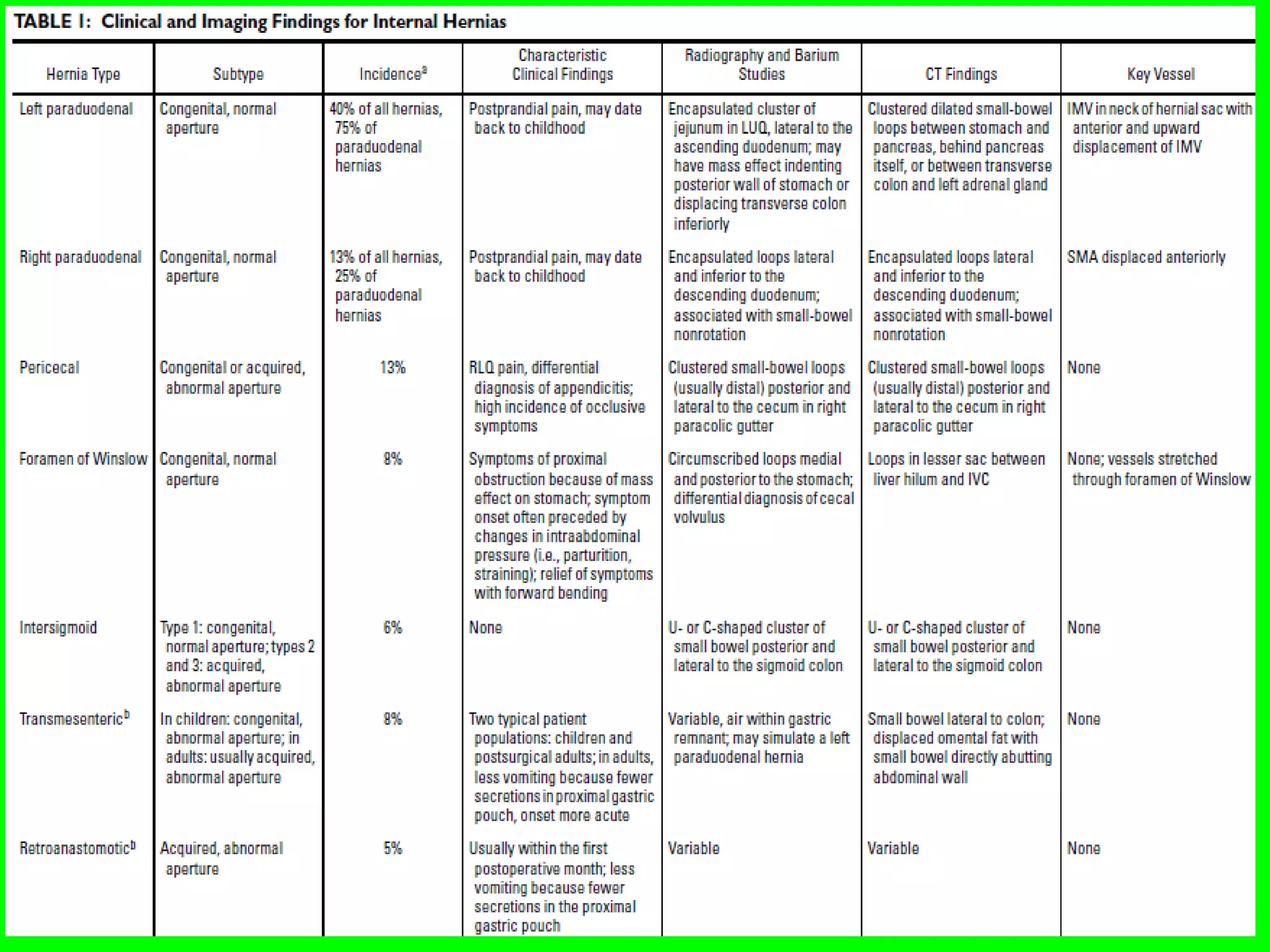

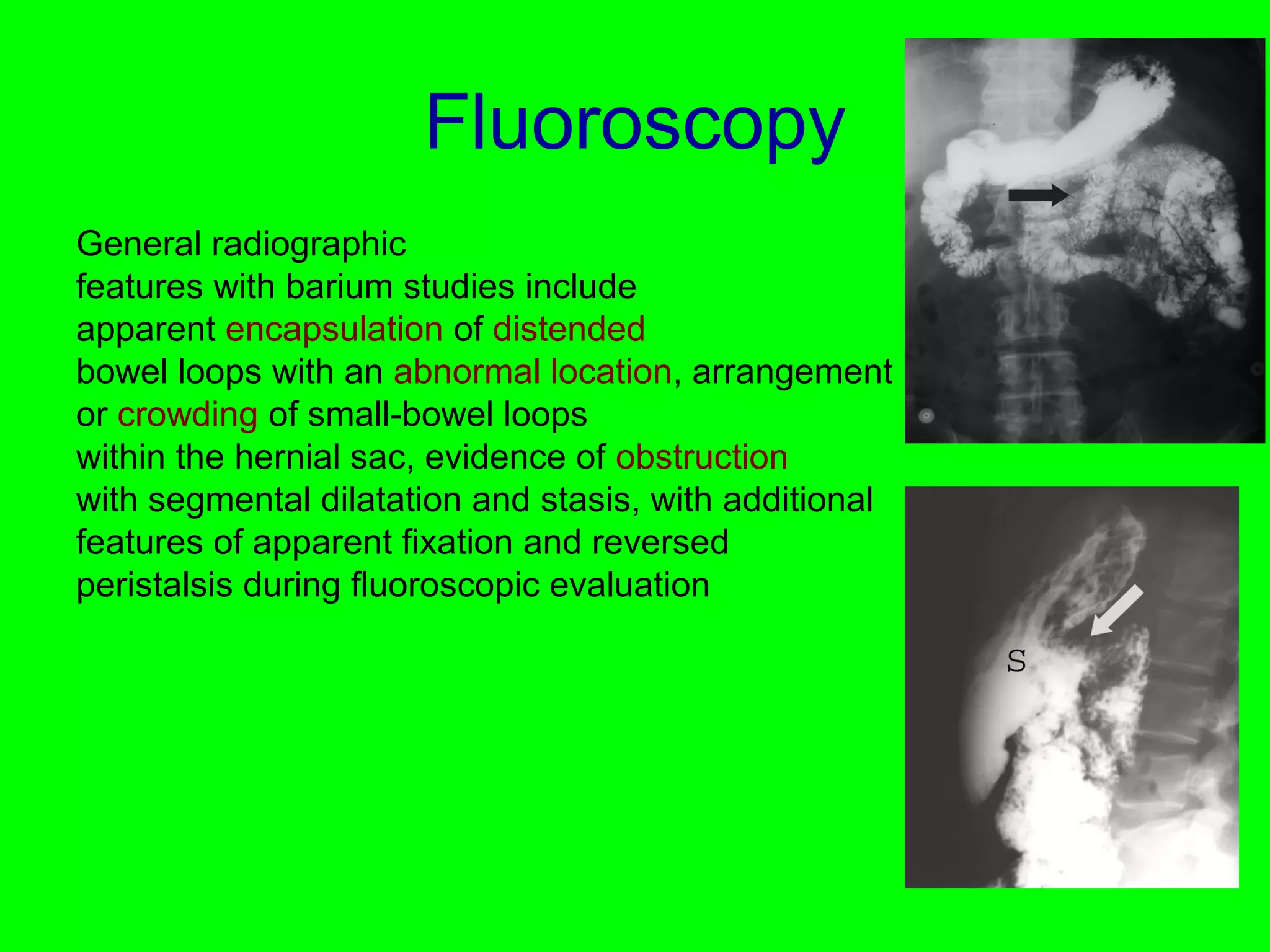
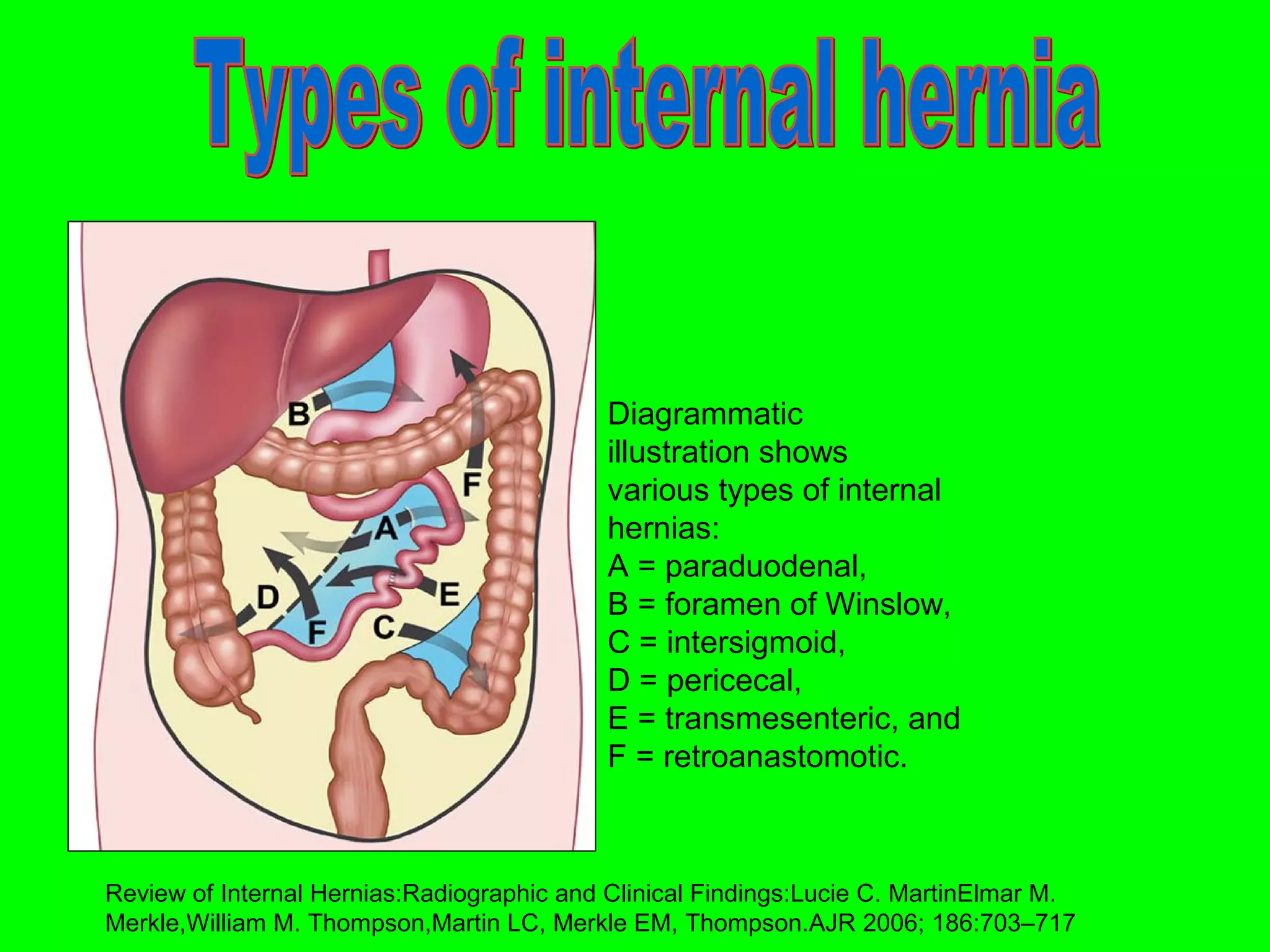
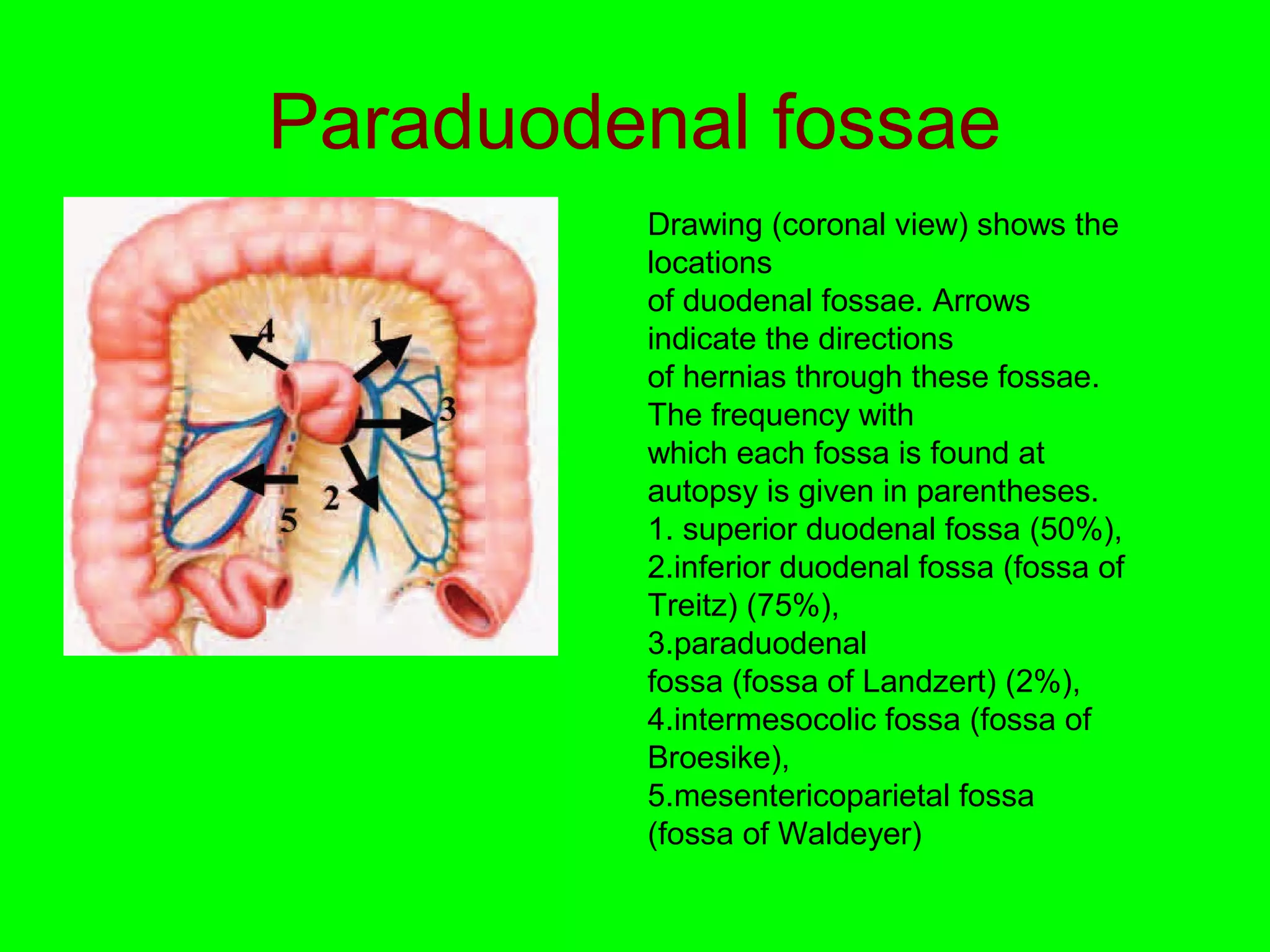
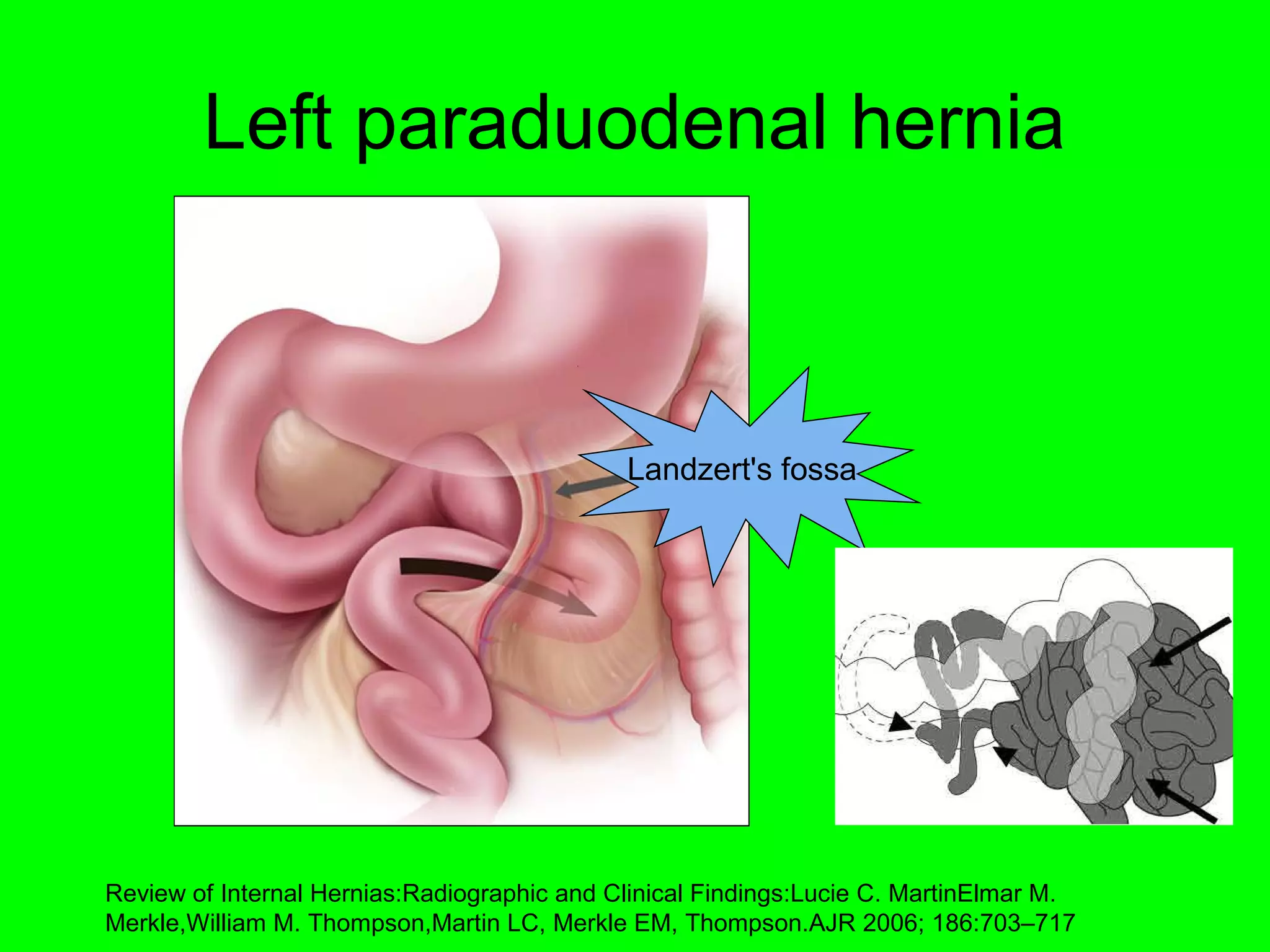
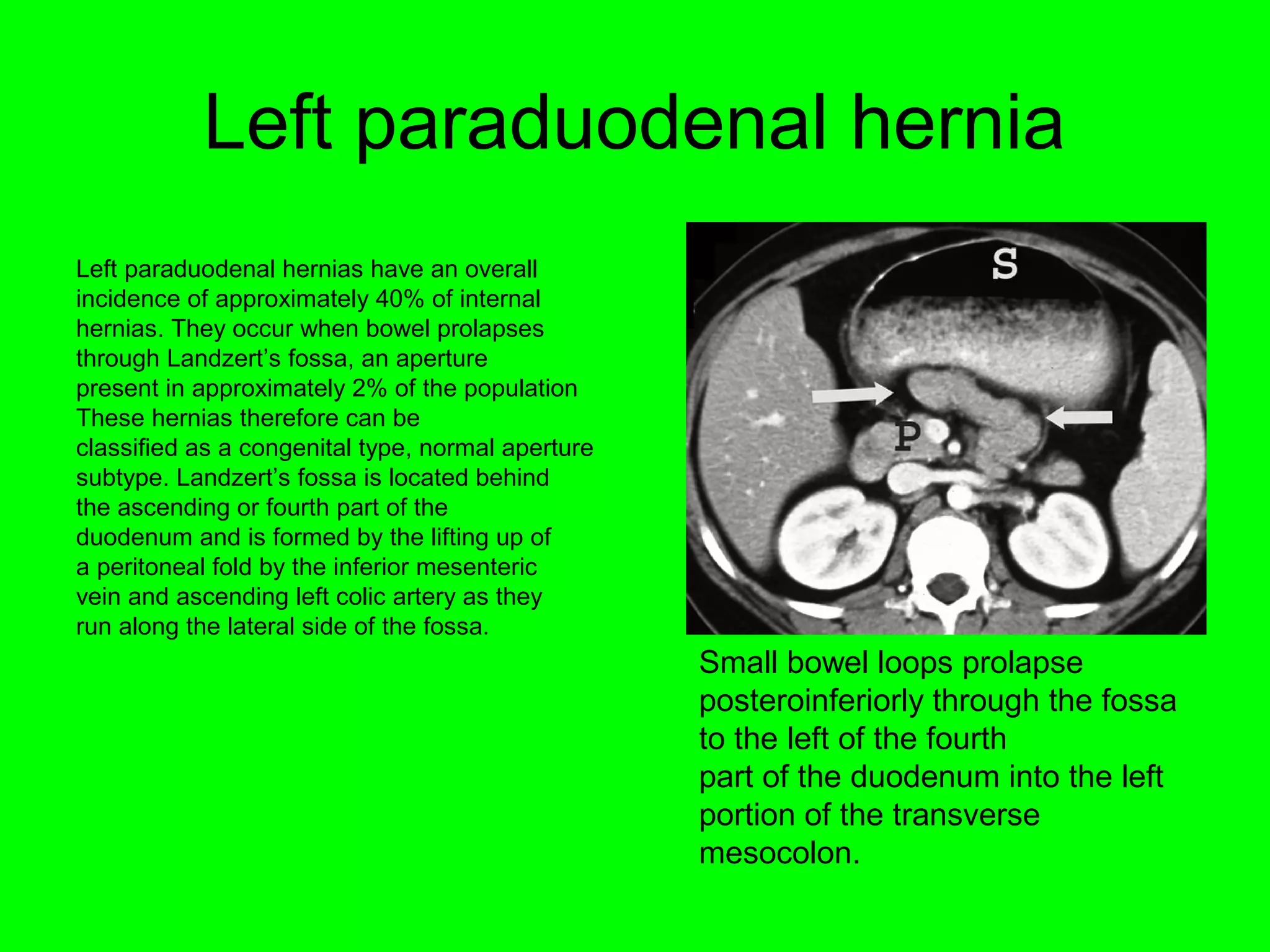
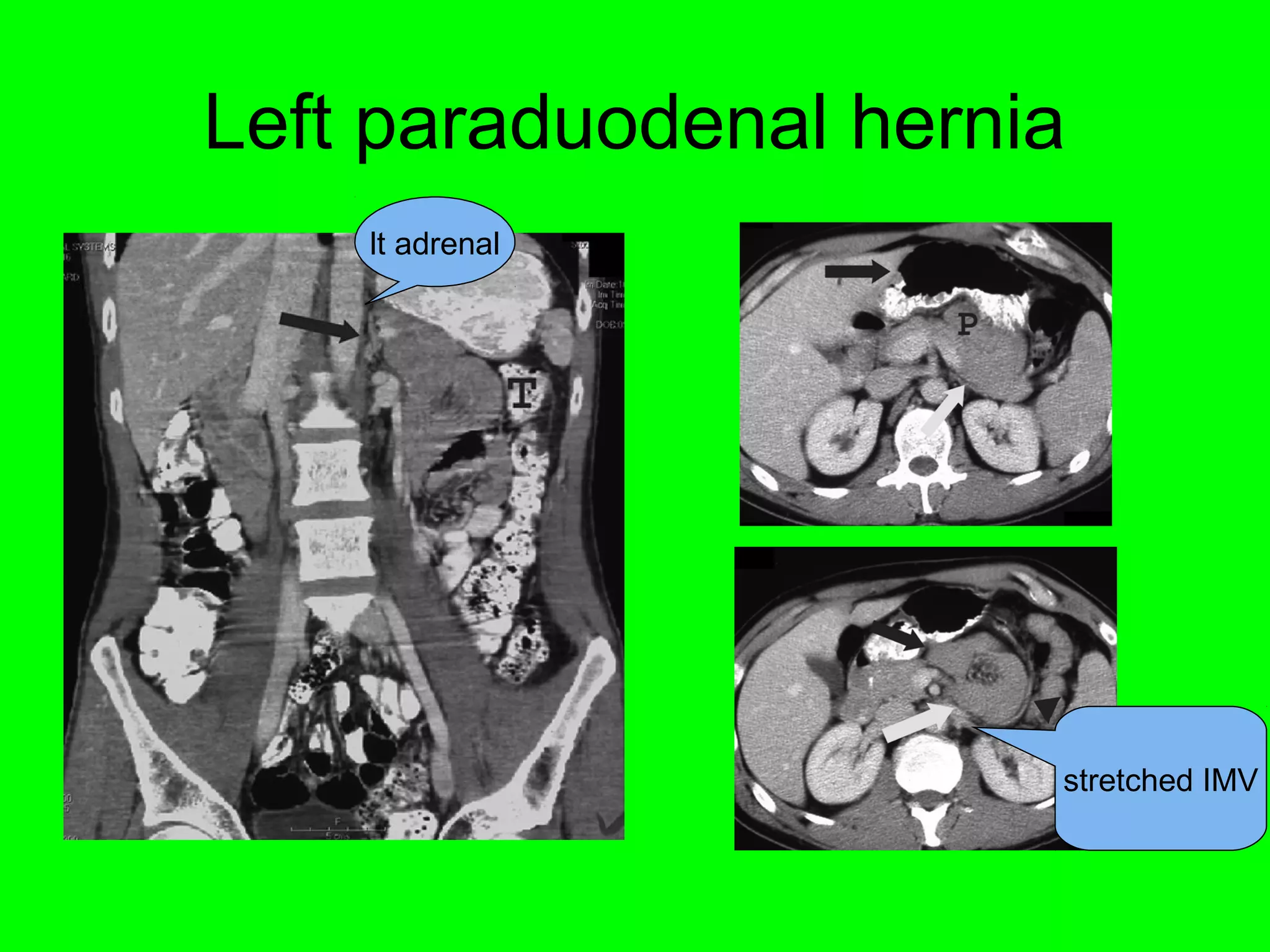
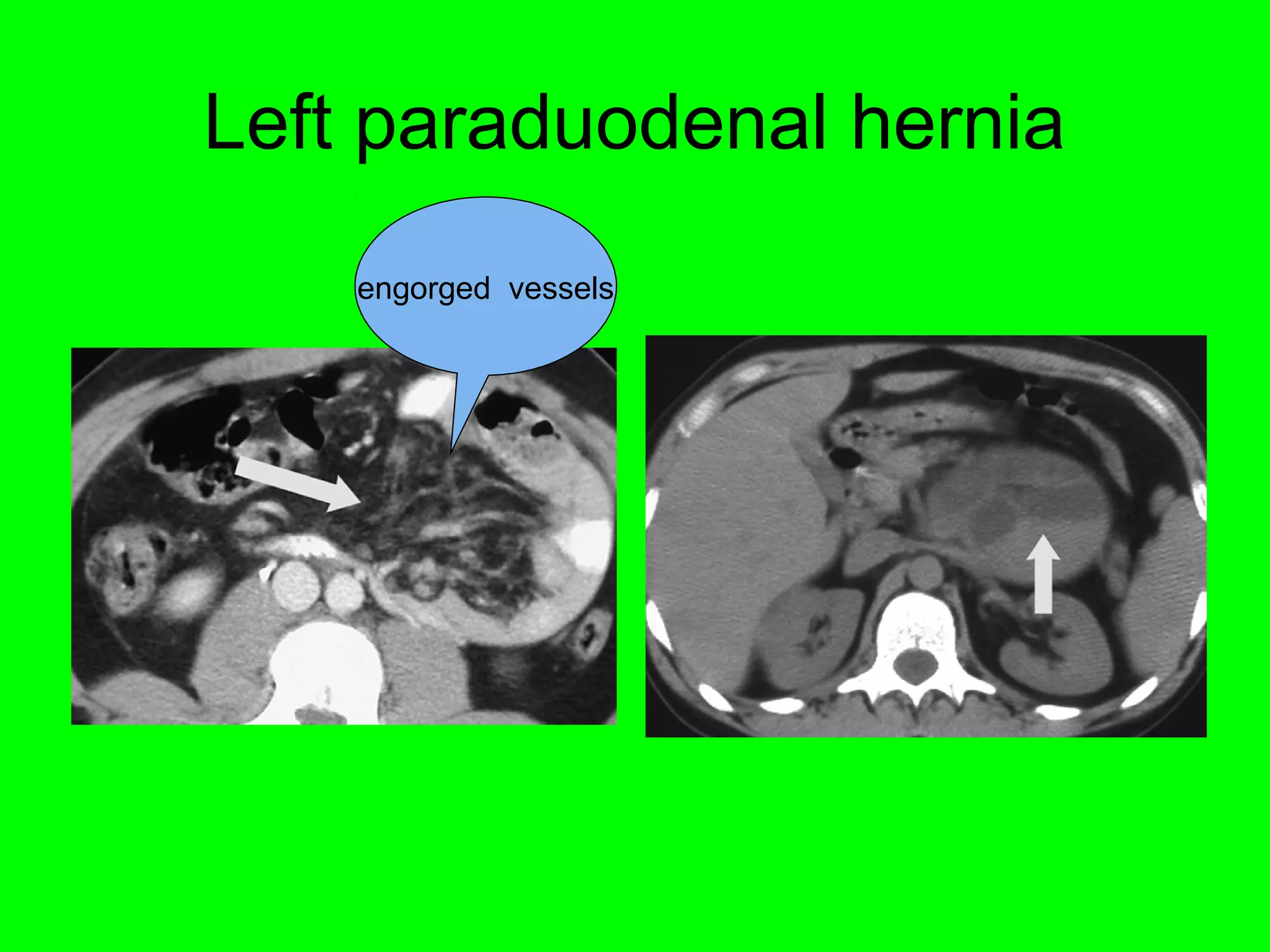
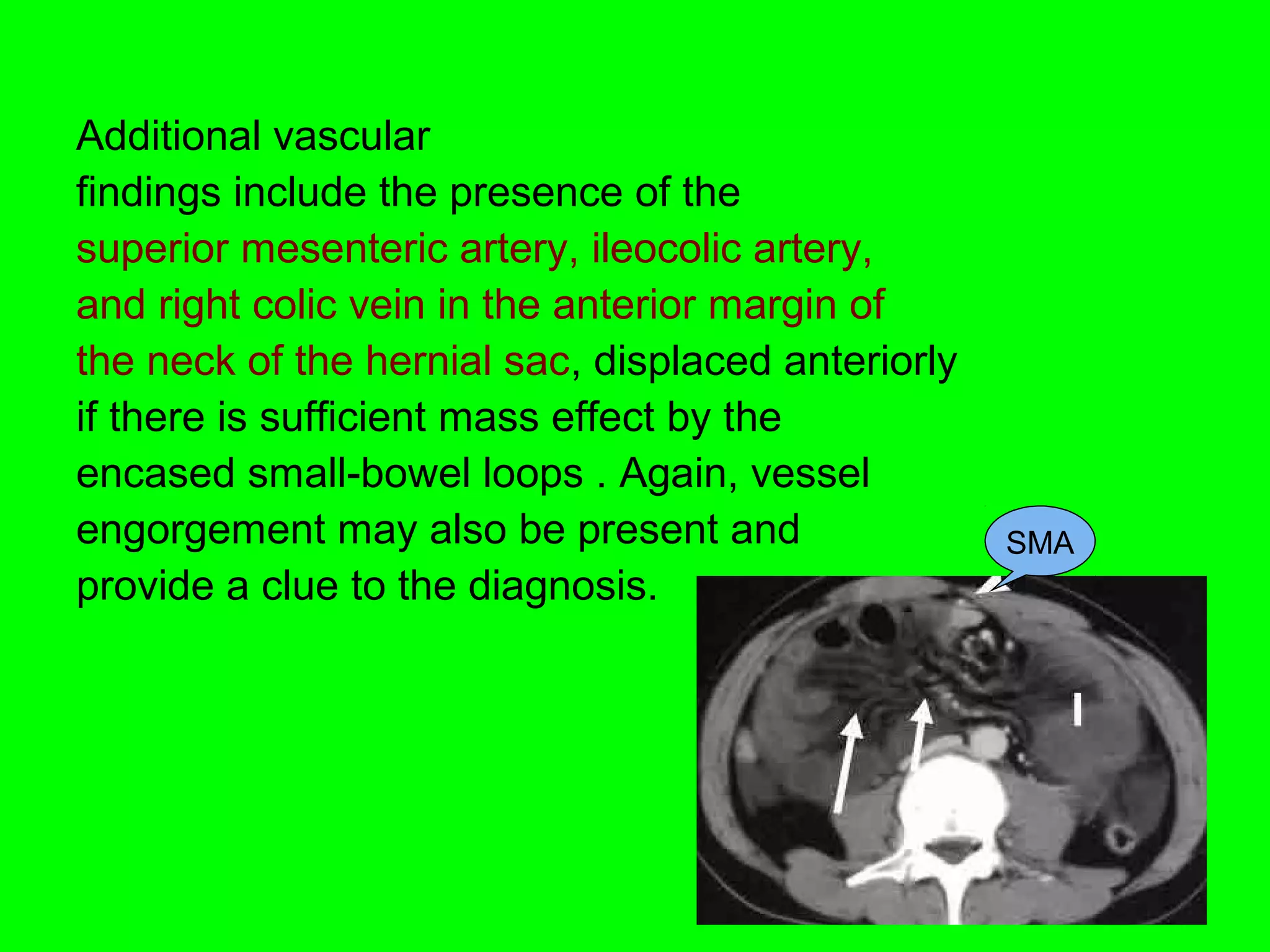
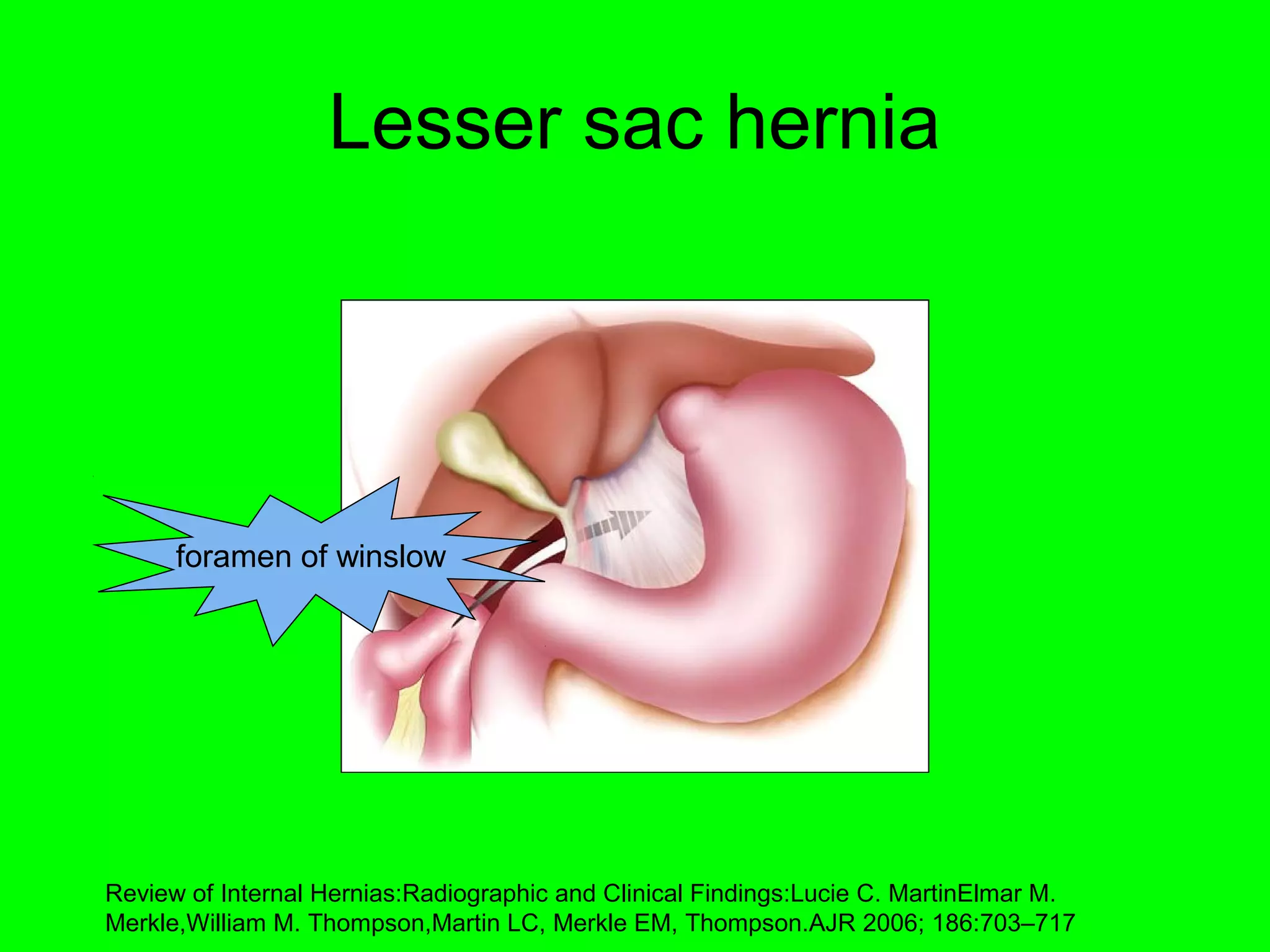
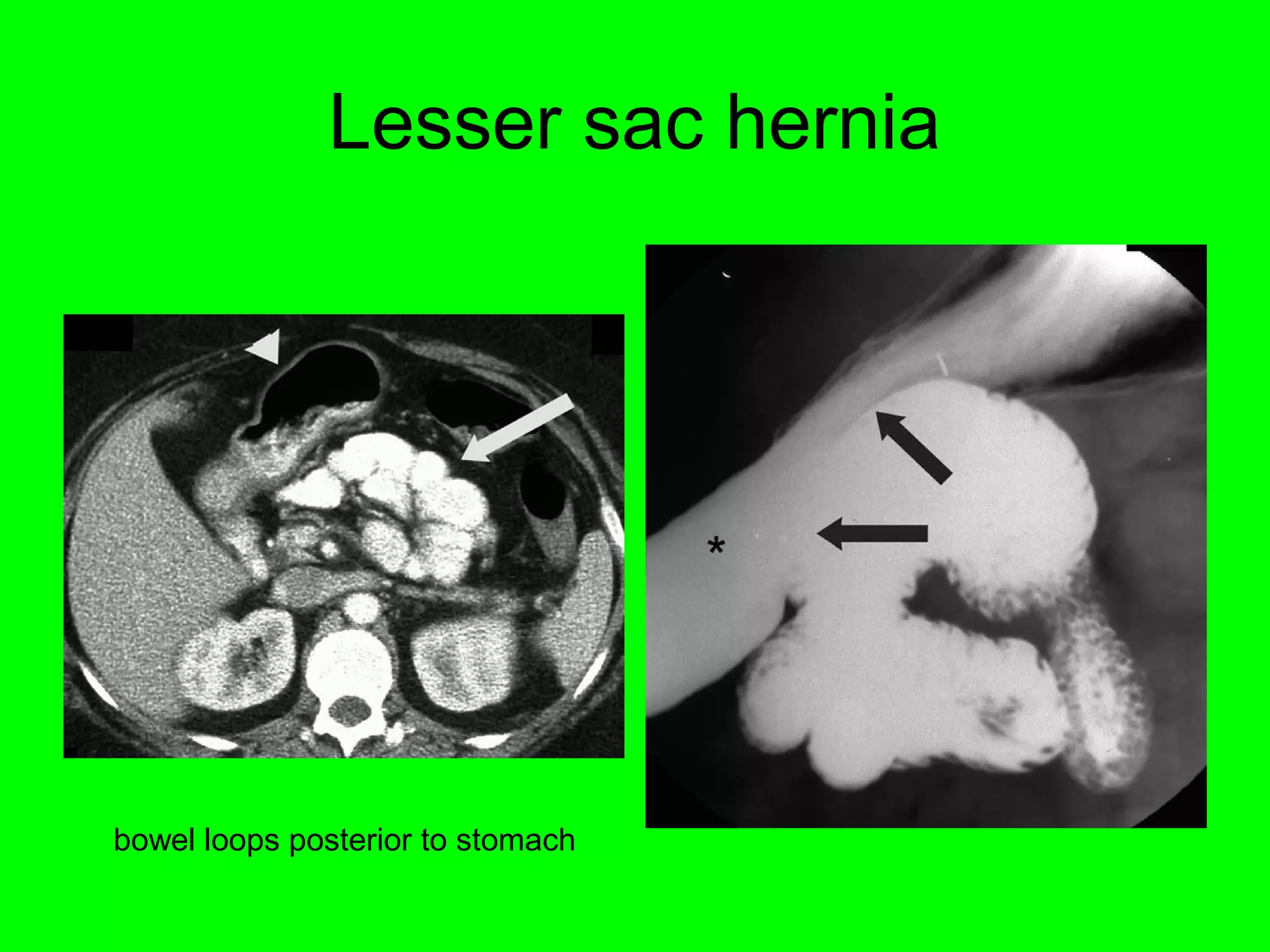
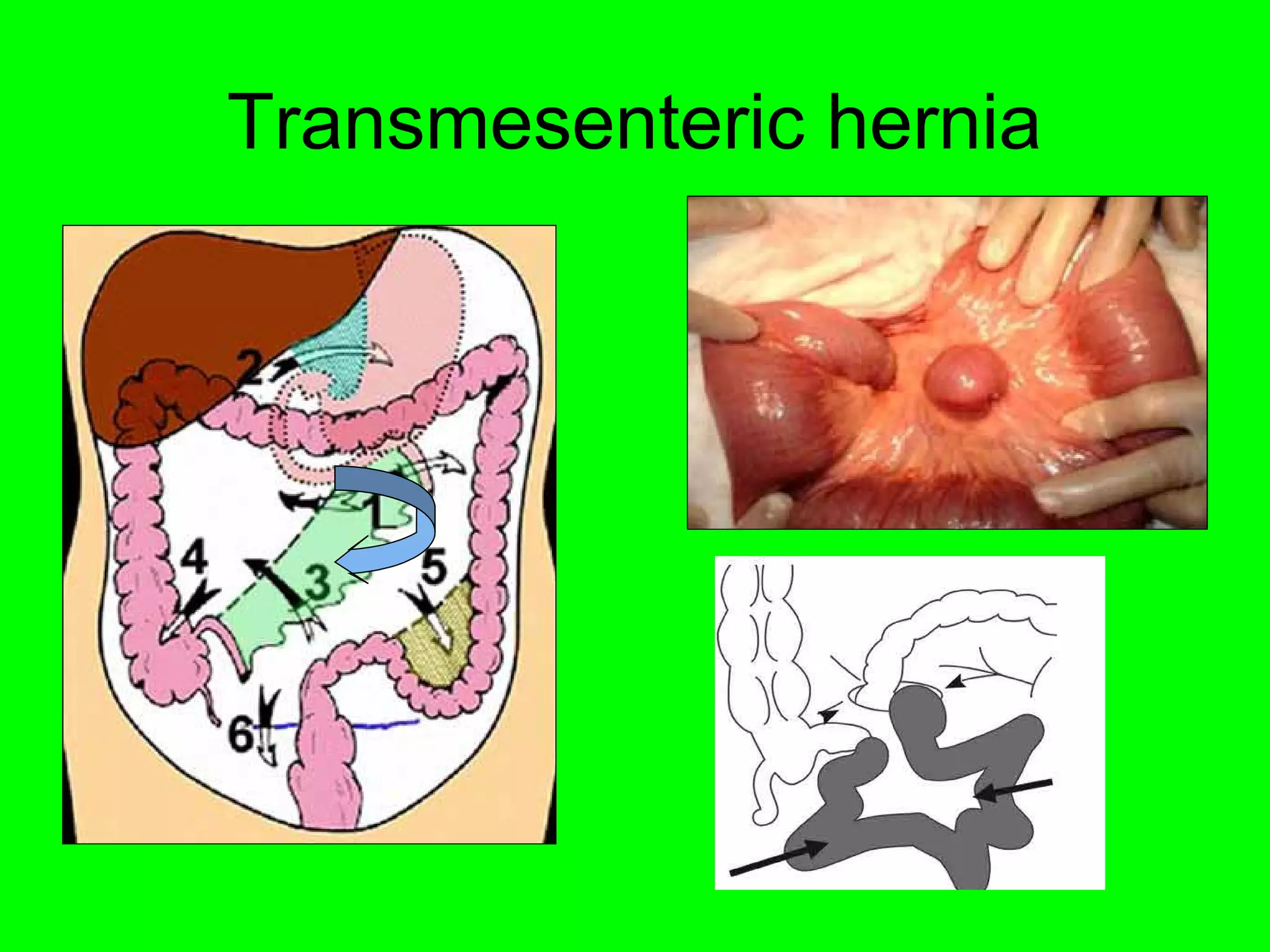
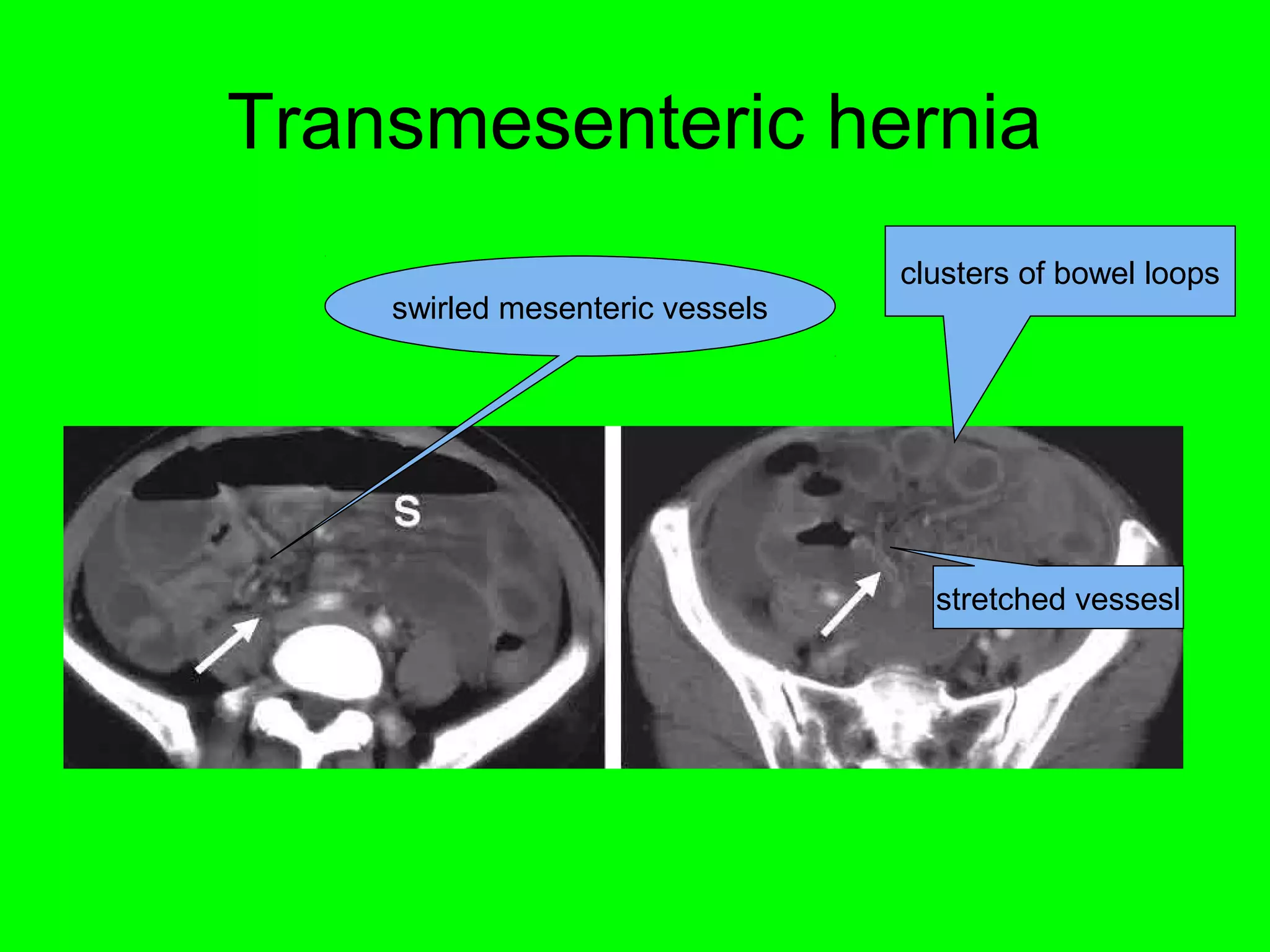
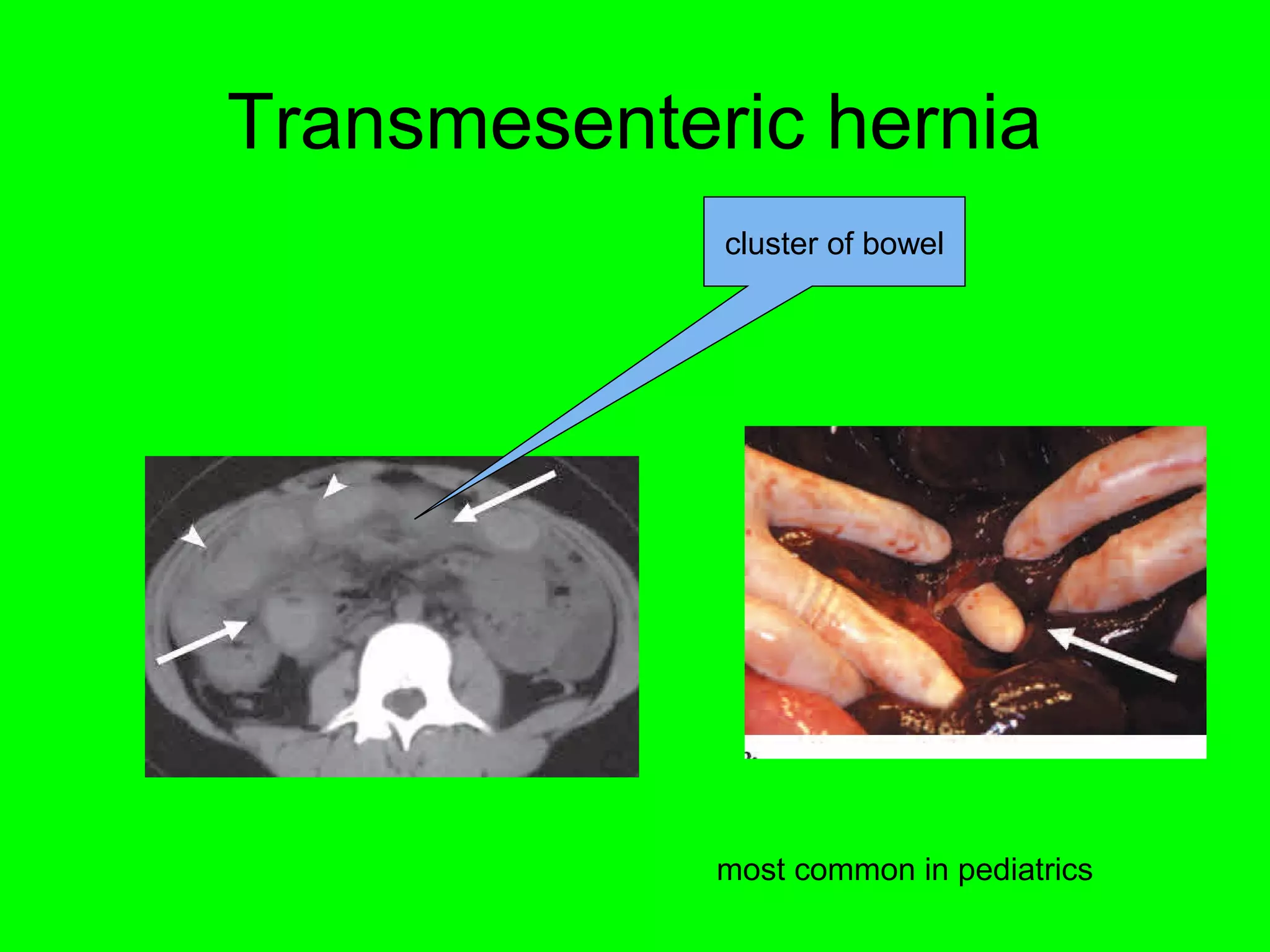
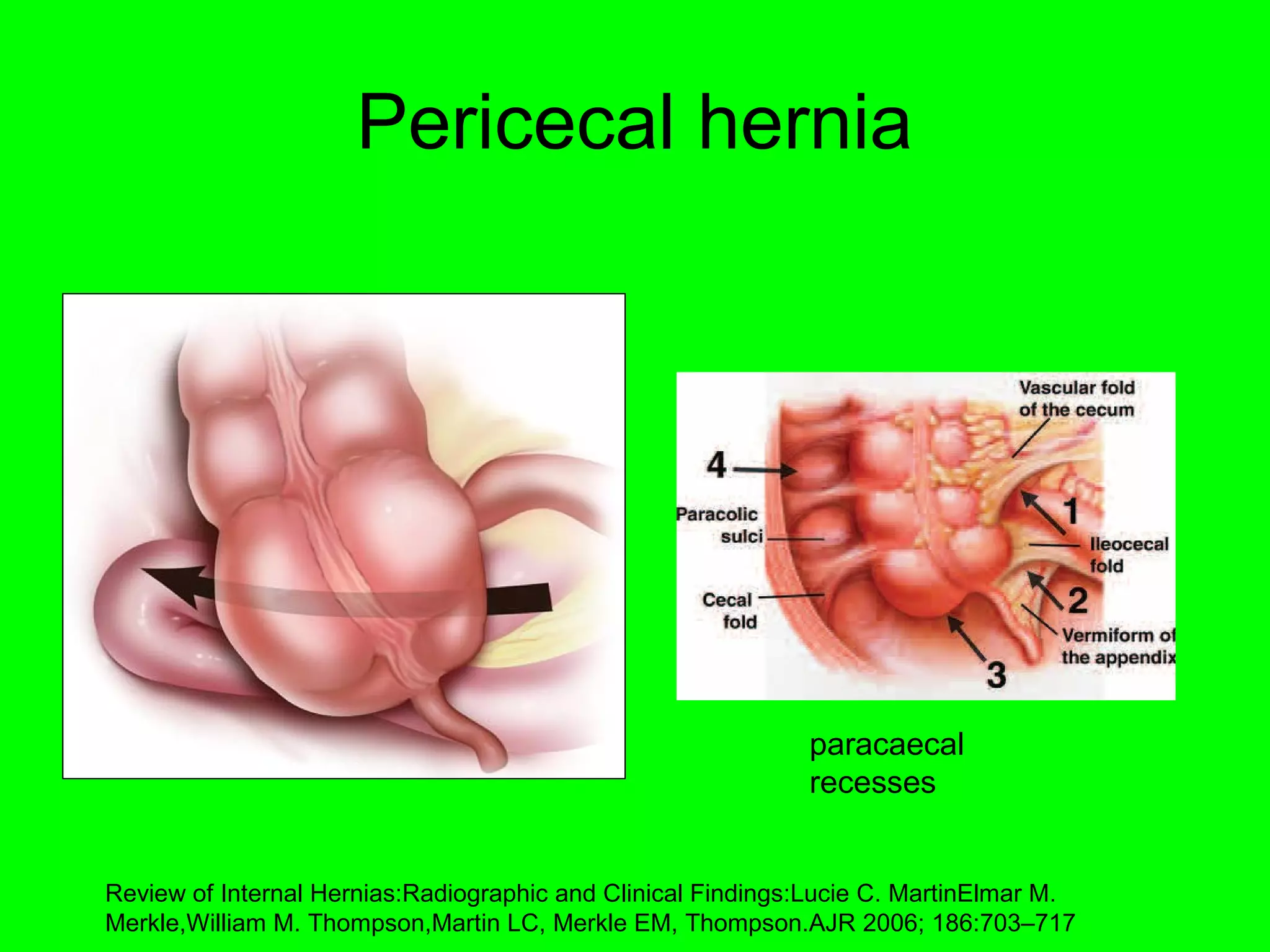
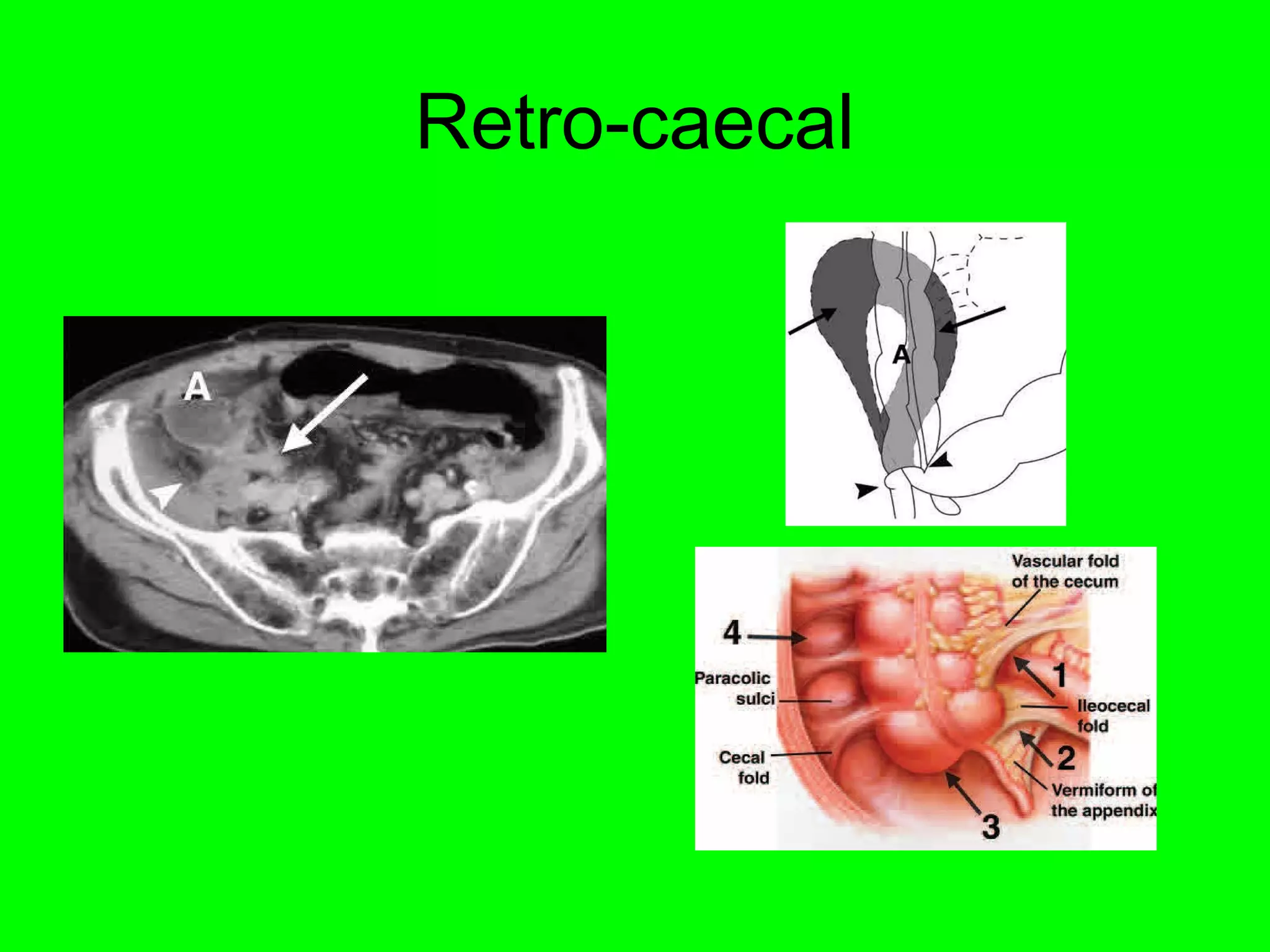
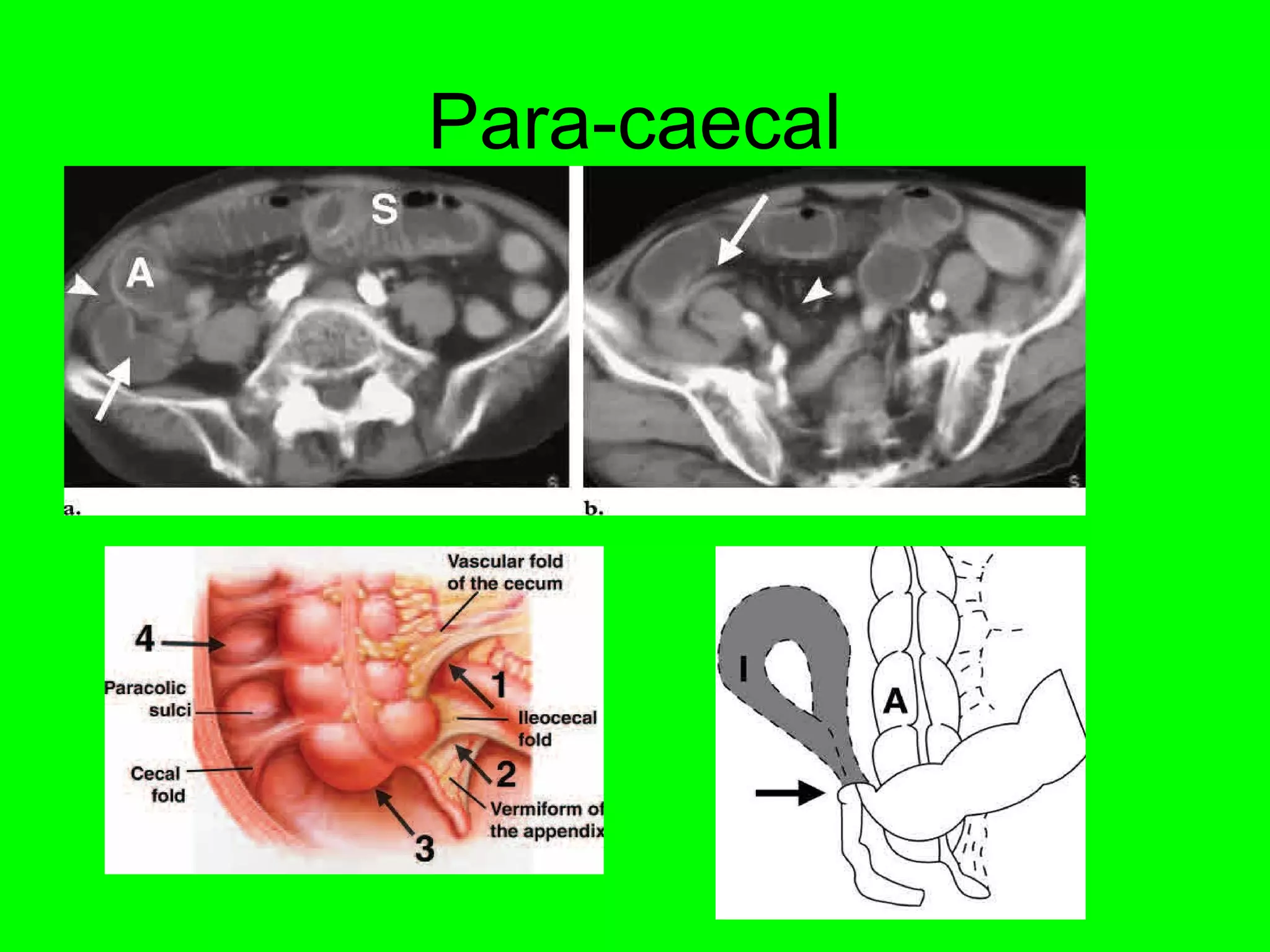
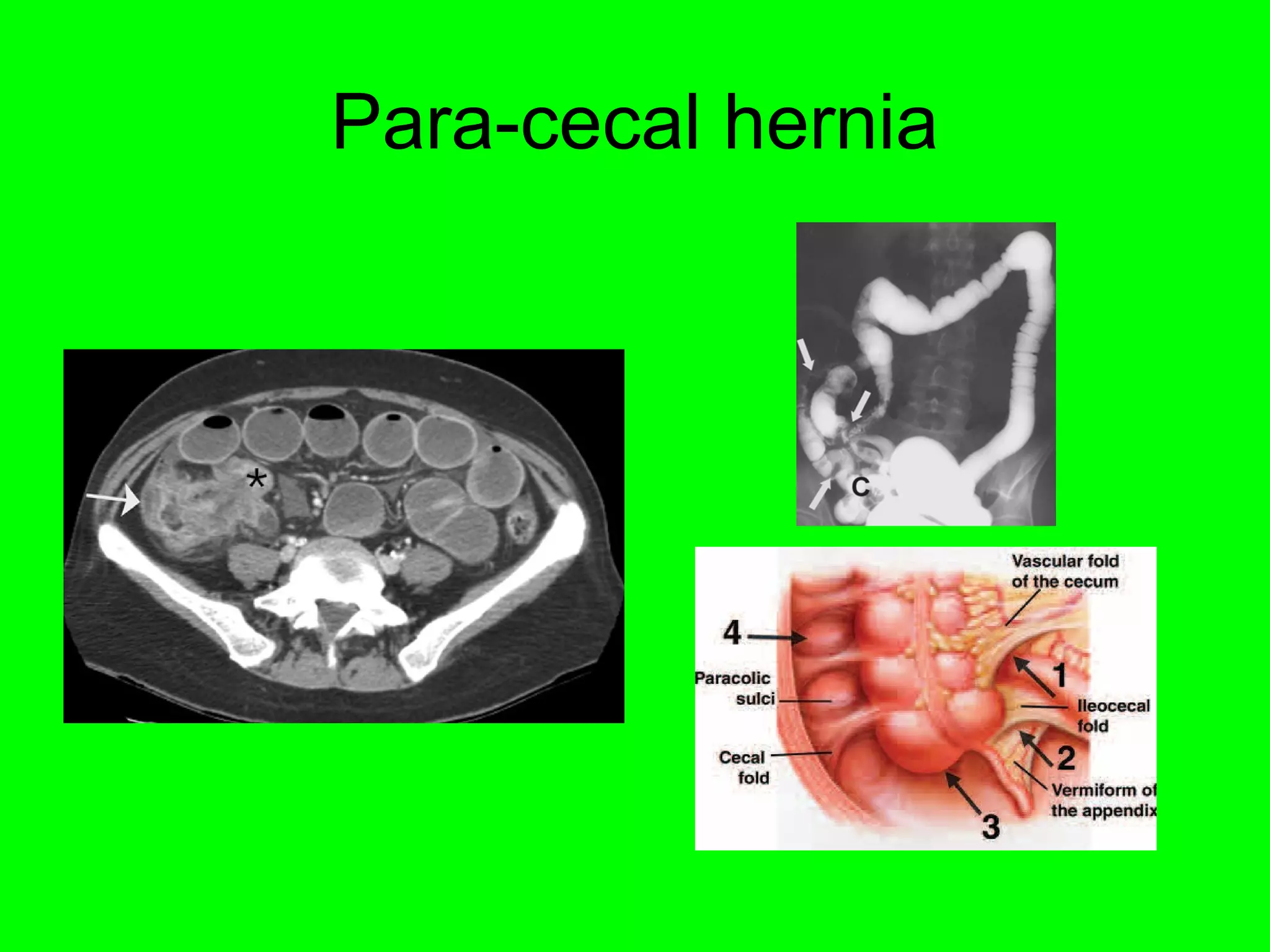
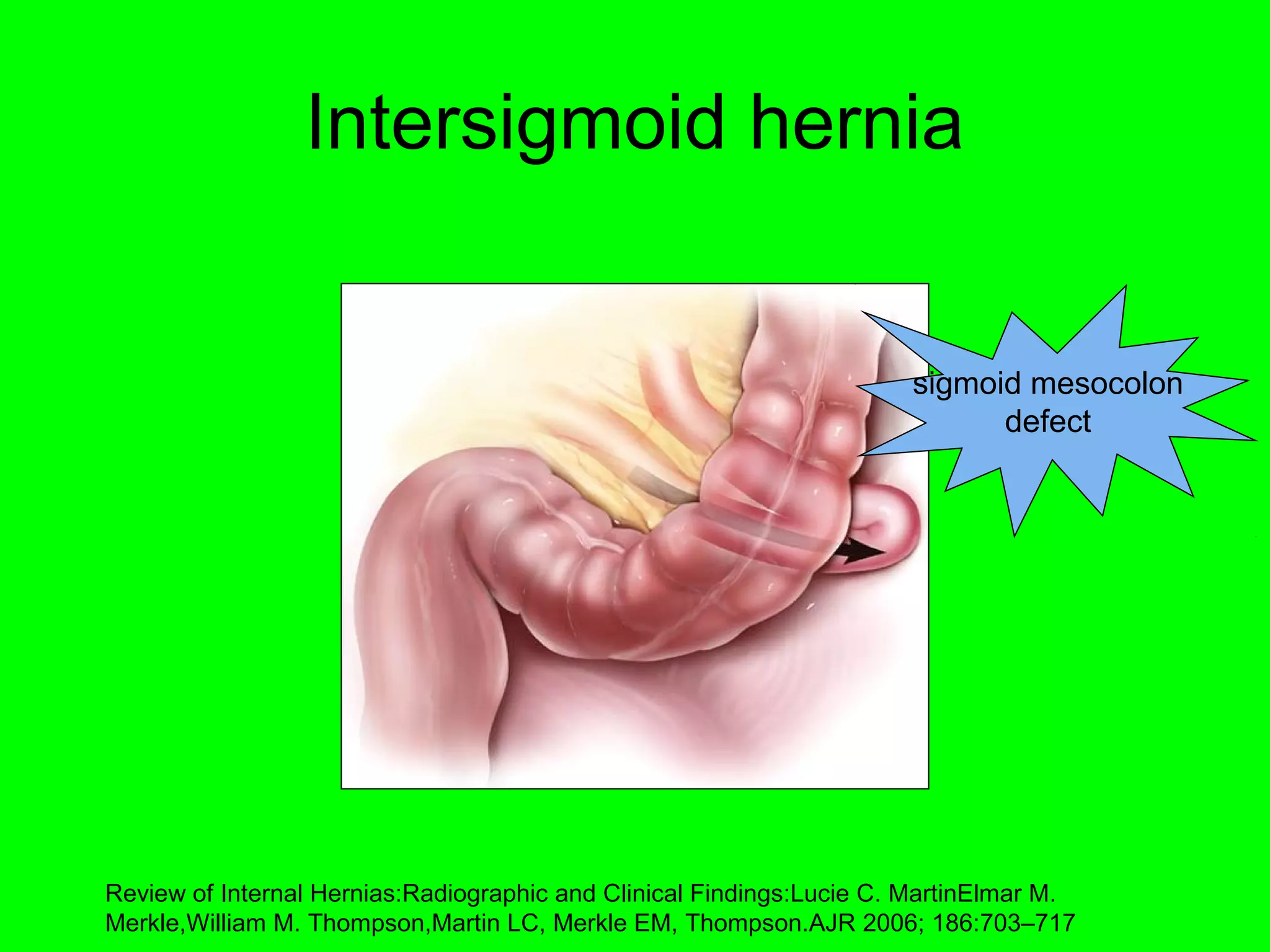
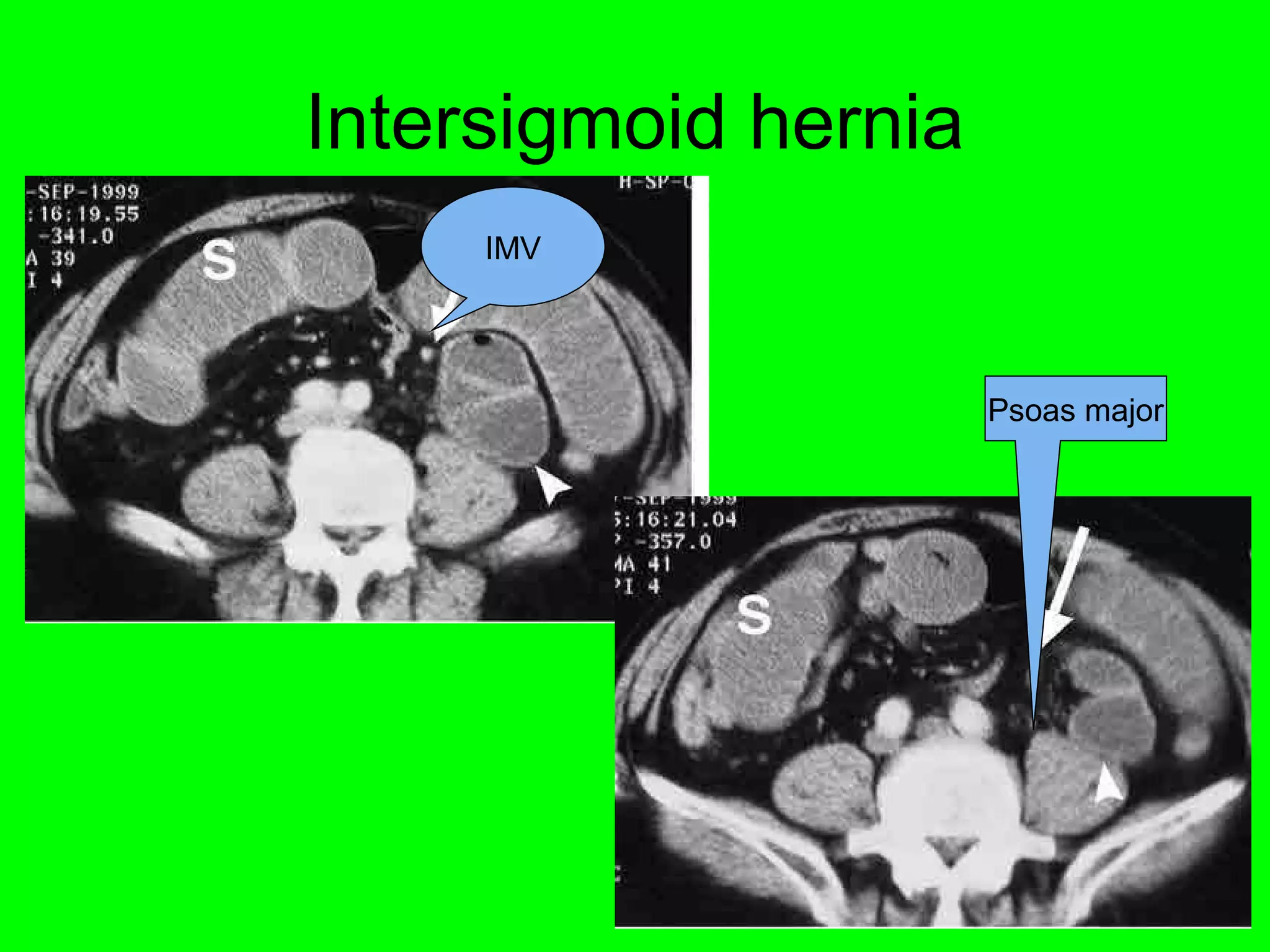
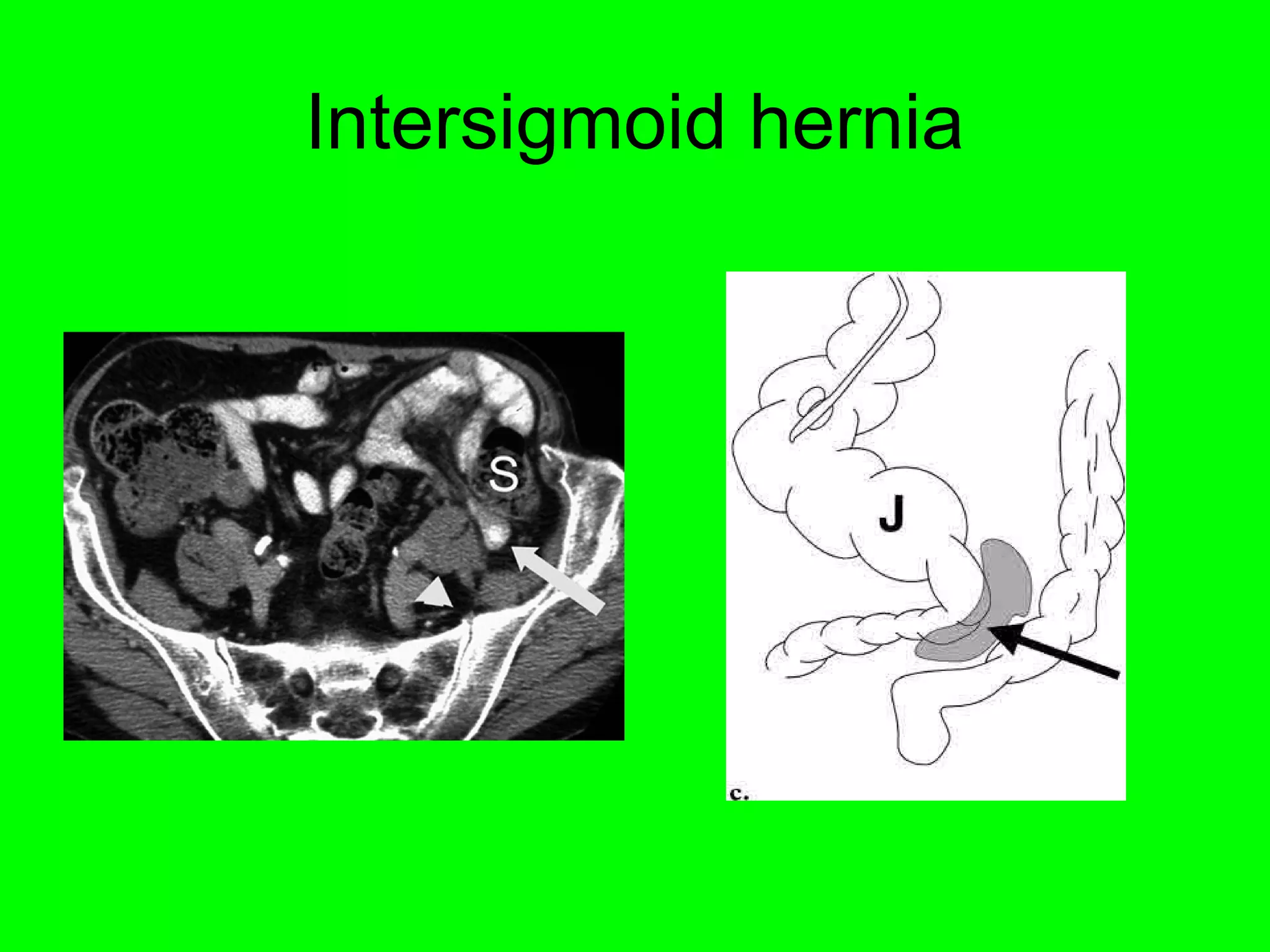
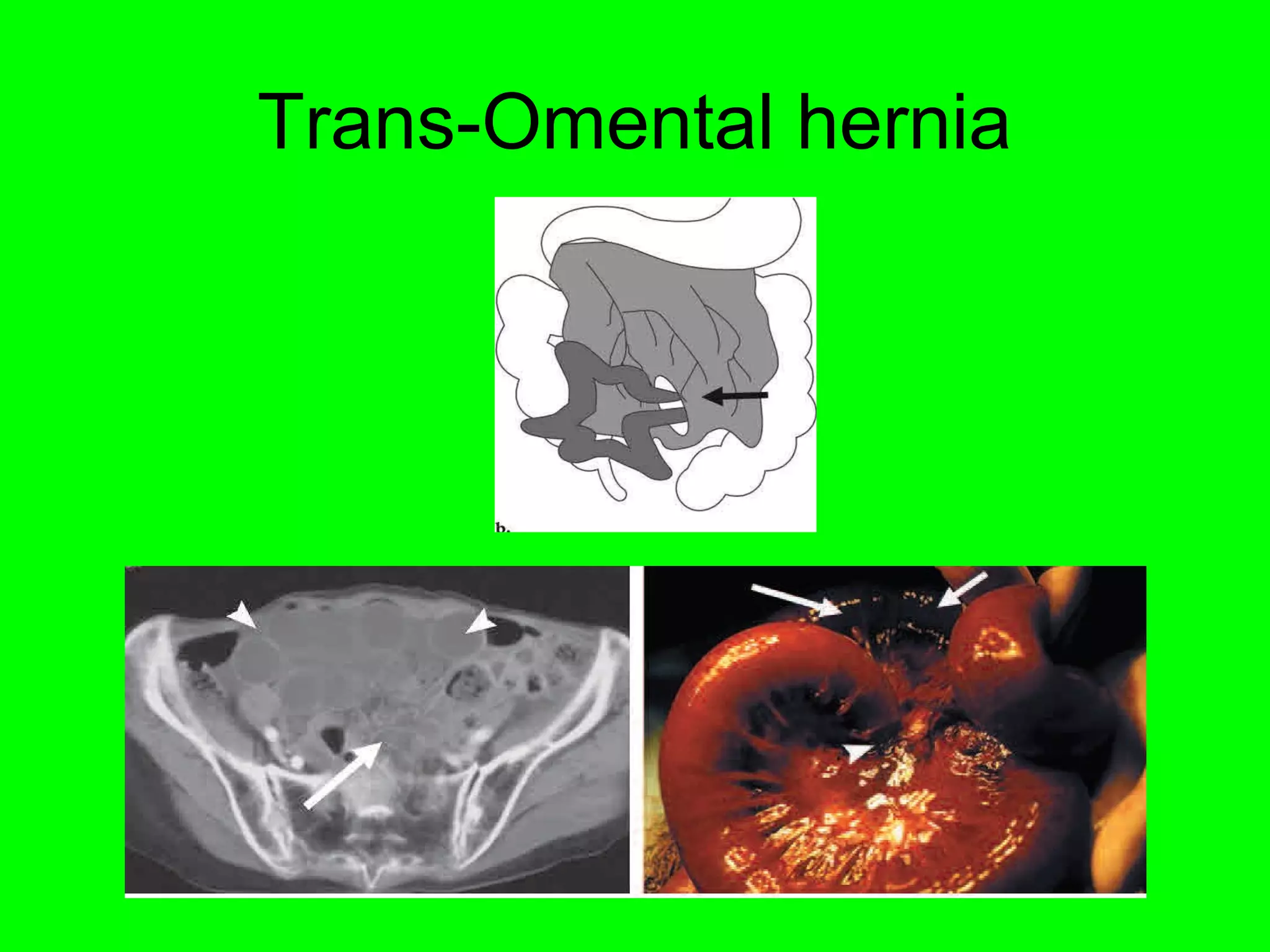
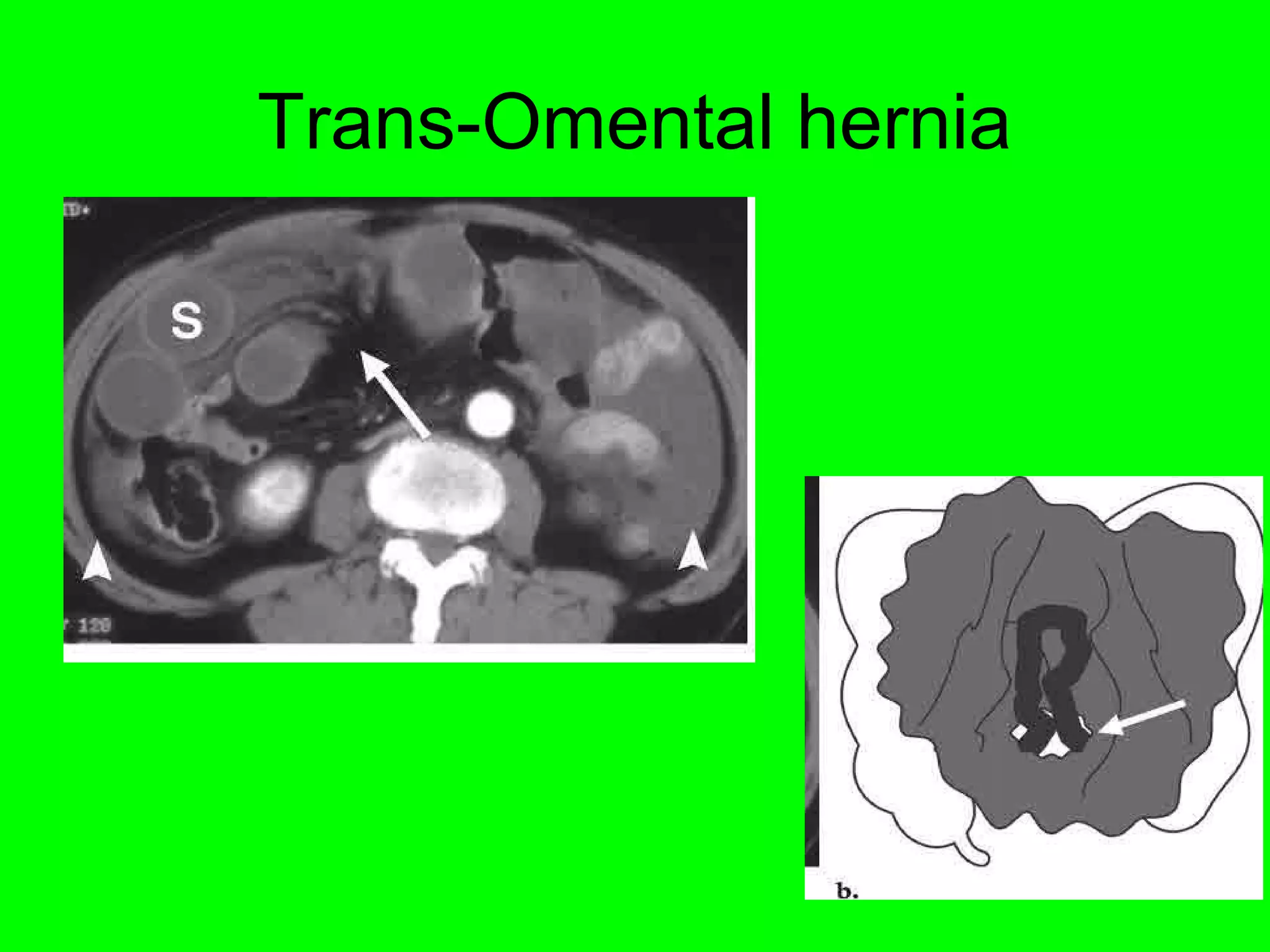
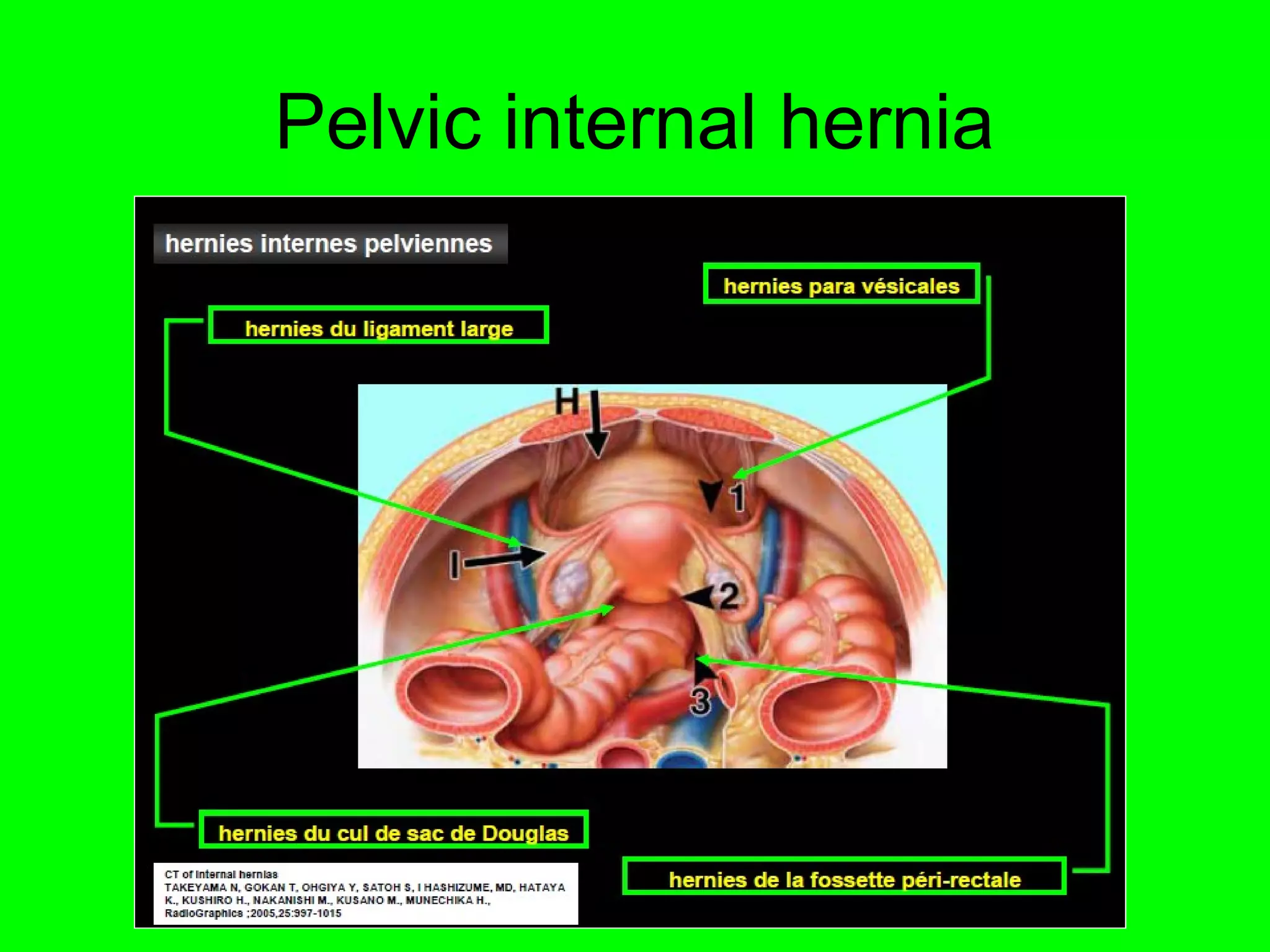
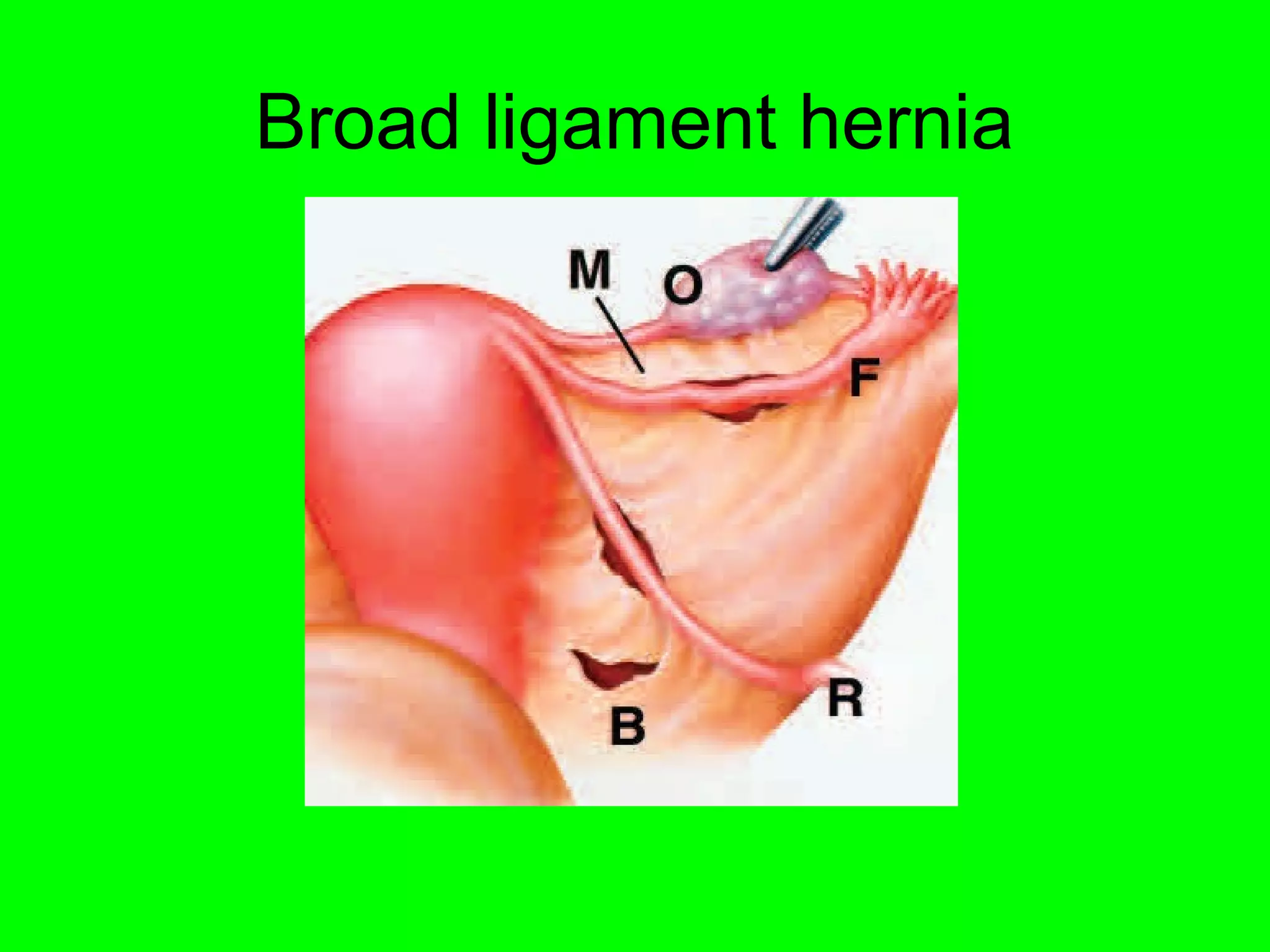
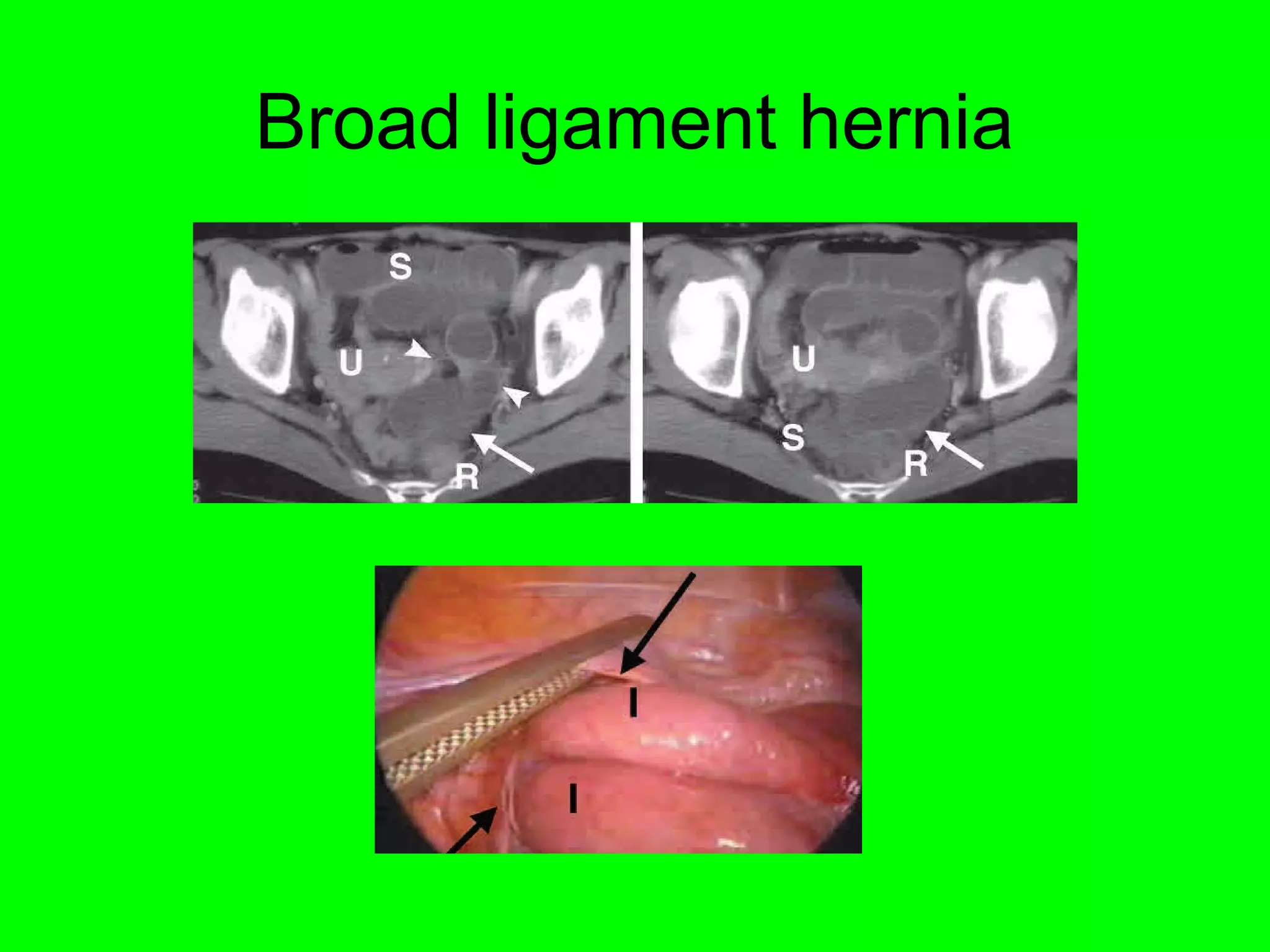
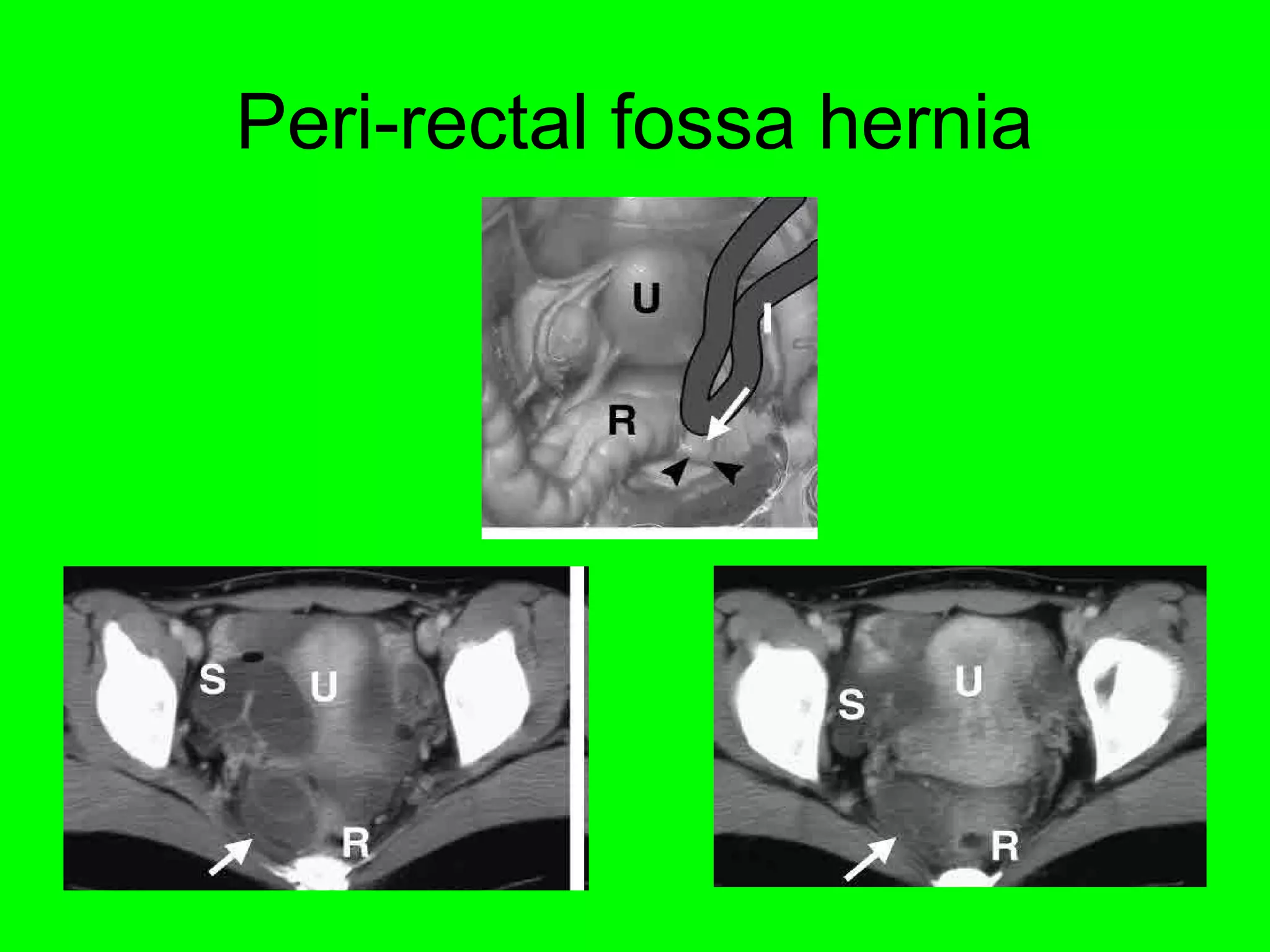
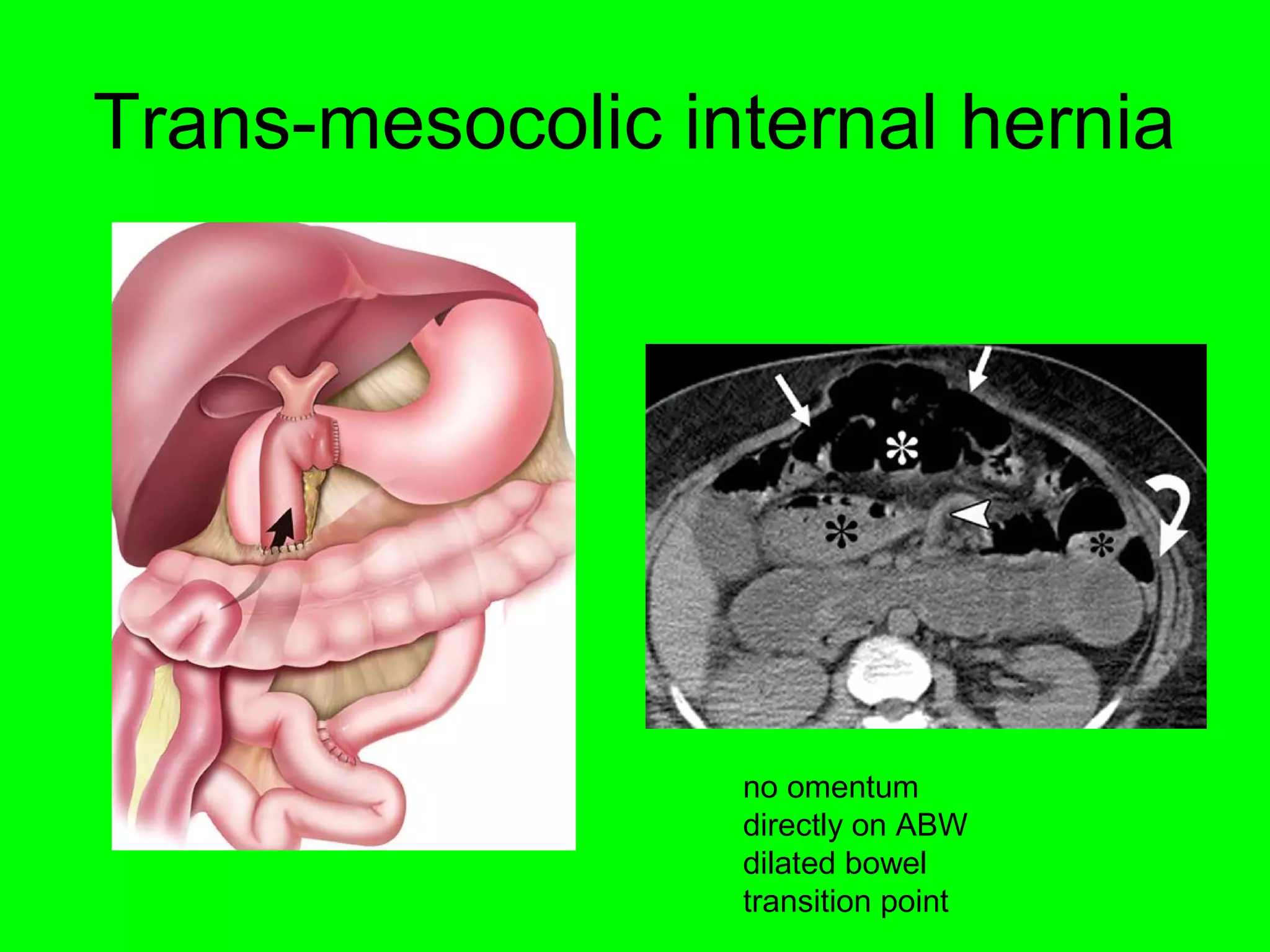
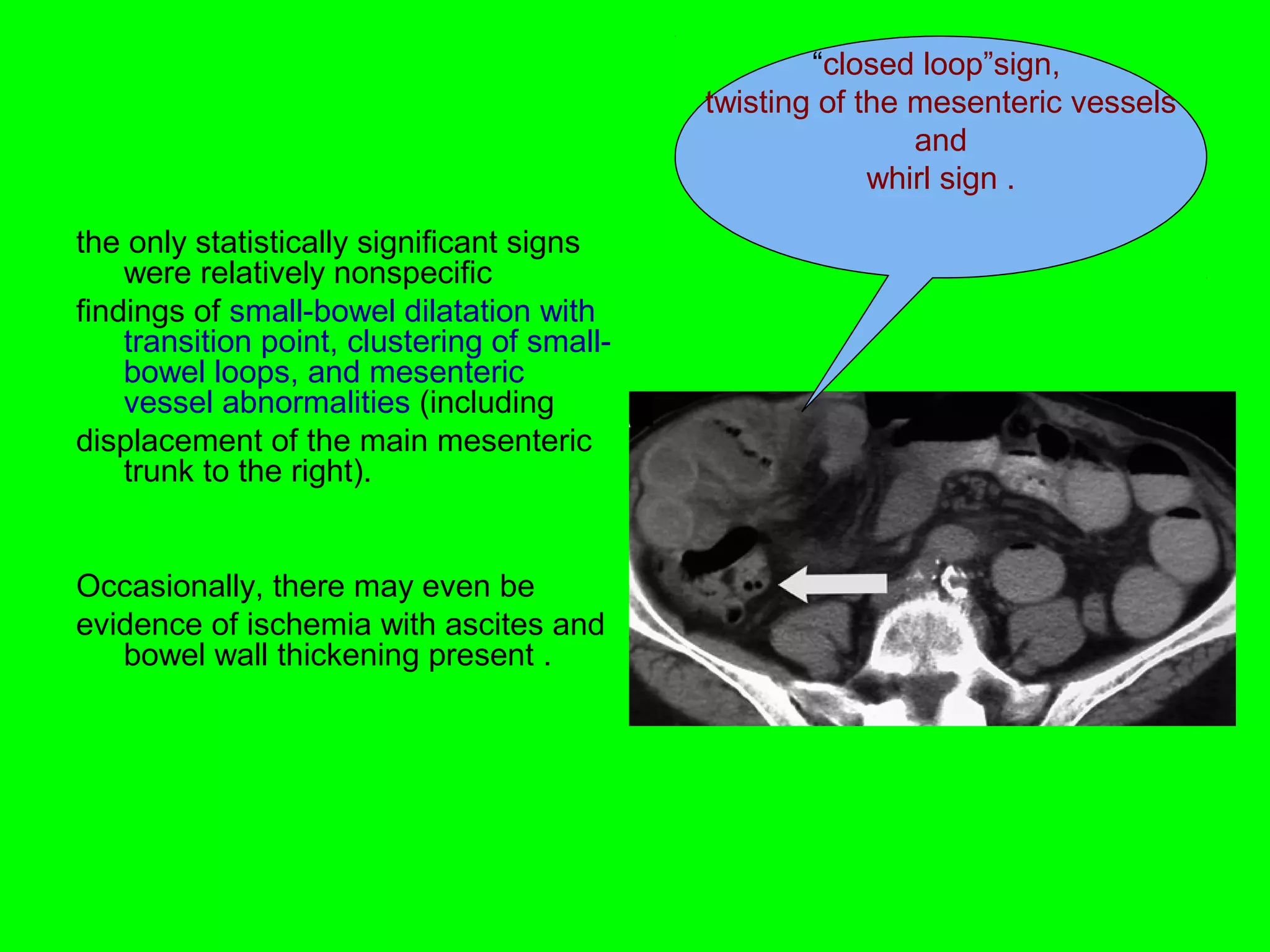



This document discusses internal hernias, which occur when abdominal organs protrude through openings within the abdominal cavity. It describes several types of internal hernias, including paraduodenal, foramen of Winslow, intersigmoid, pericecal, transmesenteric, and retroanastomotic hernias. For each type, it provides details on location, risk factors, and radiographic findings such as clustering of bowel loops and abnormalities of mesenteric vessels. The document emphasizes the importance of recognizing abnormal bowel positioning and configurations, signs of obstruction, and vessel abnormalities on imaging studies to diagnose internal hernias.











































































































