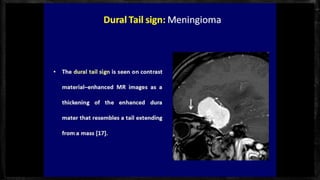
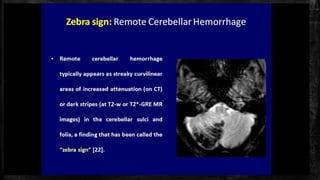
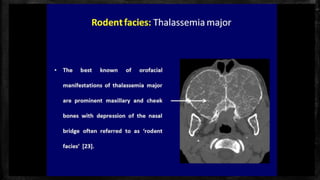
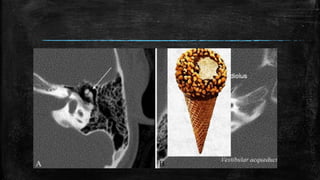
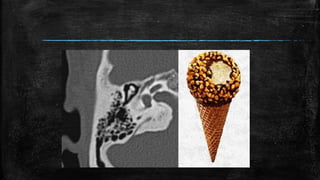
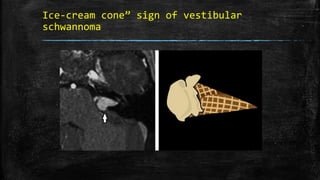
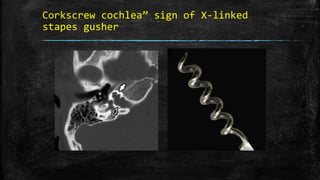
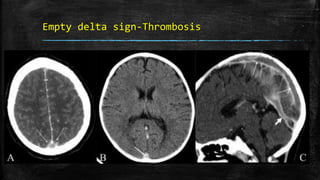
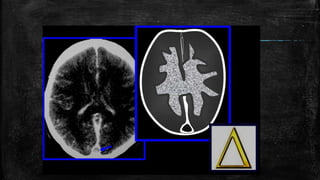
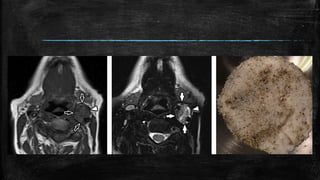
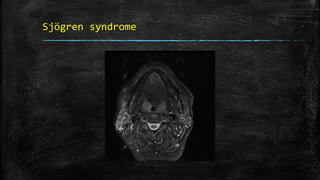
This document lists various neuroradiology signs seen on imaging and their associated medical conditions or pathologies. It includes signs such as the "ice-cream cone" sign of vestibular schwannoma, "broken heart" and "Y" signs of incudomalleolar disarticulation, "corkscrew cochlea" sign of X-linked stapes gusher, and "empty delta sign" indicating thrombosis. It also discusses signs seen in conditions like hyperparathyroidism, Sjögren syndrome, vertebral haemagioma, and more.



















































![Imaging in Neurovascular conflicts [Neurovascular compression syndrome ]](https://cdn.slidesharecdn.com/ss_thumbnails/cnv-141013092247-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)










































