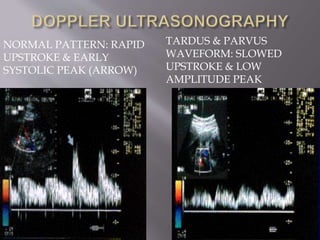
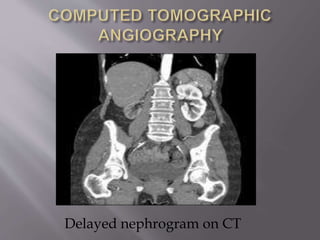
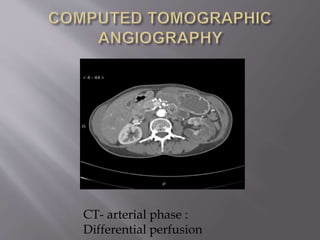
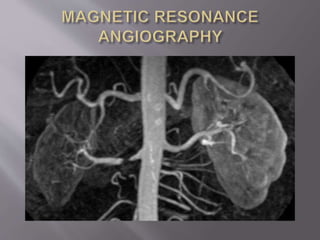
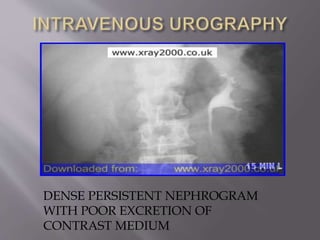
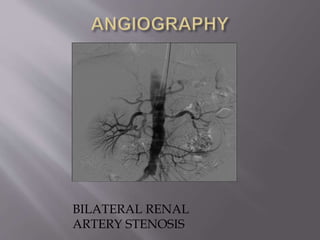
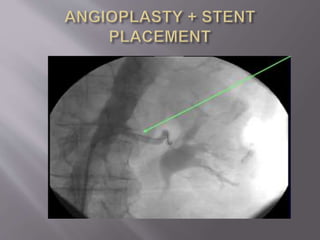
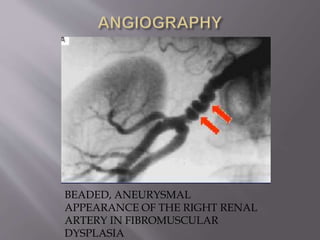
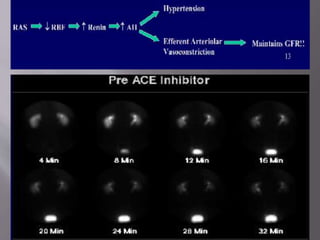
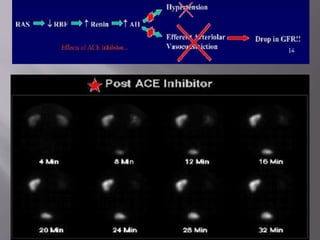
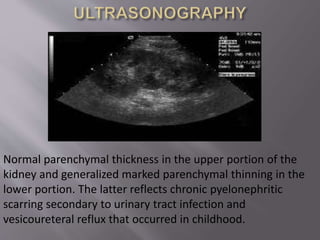
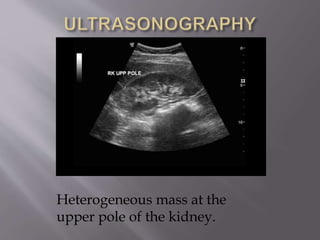
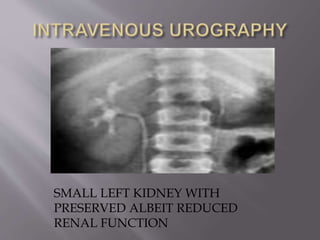
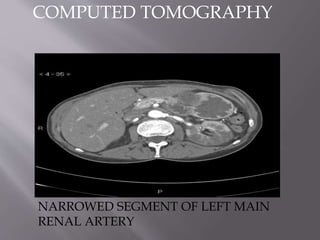
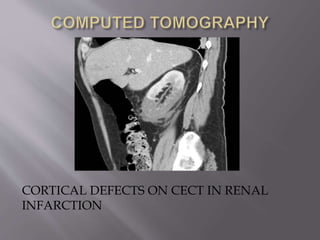
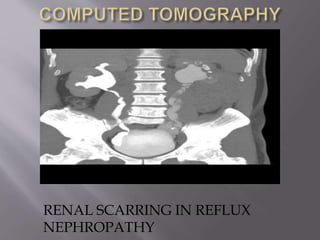
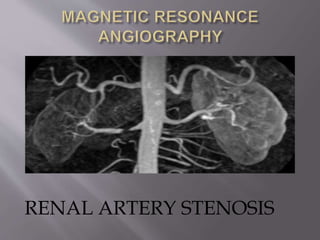
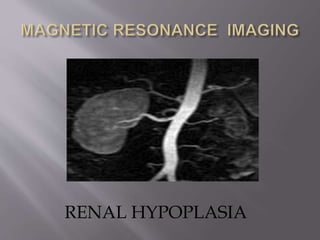
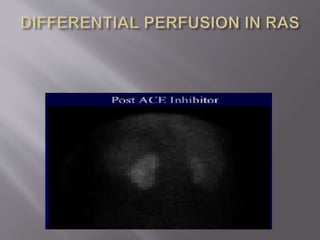
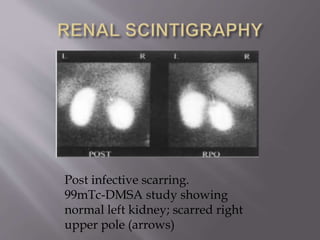
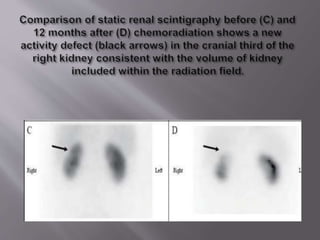
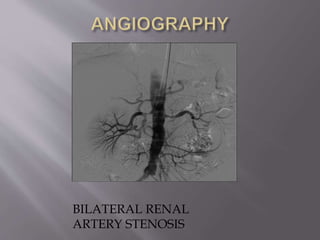
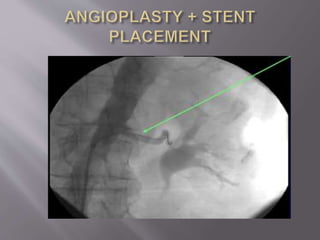
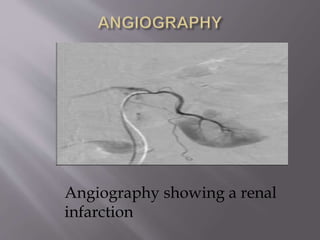
The document discusses unilateral small kidneys and the role of imaging in establishing a diagnosis. It describes various causes of unilateral small kidneys including pre-renal issues like renal artery stenosis, intra-renal issues such as renal infarction, and post-renal issues like reflux nephropathy. Imaging modalities like ultrasound, CT, MRI, renal scintigraphy, and angiography are discussed for evaluating the kidneys and determining the underlying etiology. The document emphasizes how different imaging findings can help identify conditions that may cause one kidney to be smaller than the other.