Downloaded 597 times







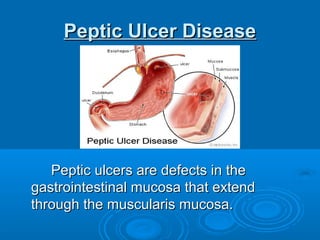






Acid peptic disorders include gastroesophageal reflux disease (GERD) and peptic ulcer disease. GERD is defined as chronic symptoms or mucosal damage caused by abnormal reflux of gastric contents into the esophagus. Peptic ulcers are defects in the gastrointestinal mucosa that extend through the muscularis mucosa. Common causes of peptic ulcers include Helicobacter pylori infection and NSAID use. Treatment involves eradicating H. pylori, discontinuing NSAIDs, and using proton pump inhibitors, H2 receptor antagonists, or prostaglandins to promote healing.











































































































