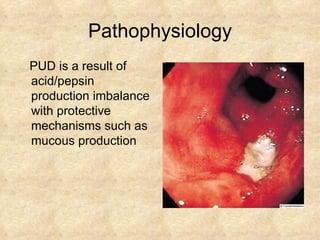
This document discusses peptic ulcer disease (PUD), including risk factors, pathophysiology, diagnosis, and treatment. Some key points:
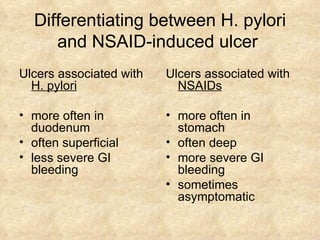
- H. pylori infection and NSAID use are the leading causes of PUD. H. pylori infection is present in 60% of Americans over age 60.
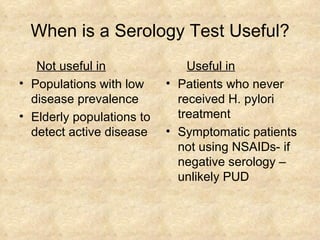
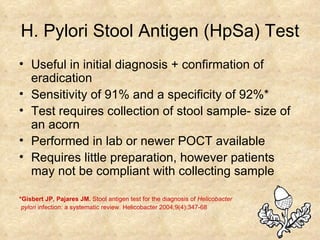
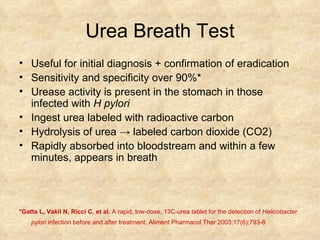
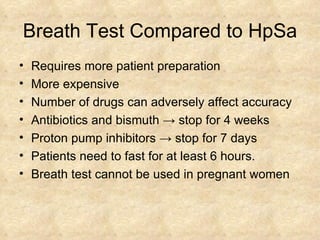
- Diagnosis involves testing for H. pylori (stool antigen, urea breath, serology), and endoscopy if high risk or symptoms persist after treatment.
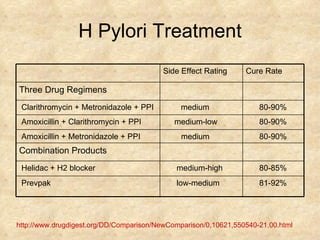
- Treatment for H. pylori-associated PUD is triple therapy (PPI plus two antibiotics) for 14 days. NSAID-associated PUD is treated with PPIs and prostag