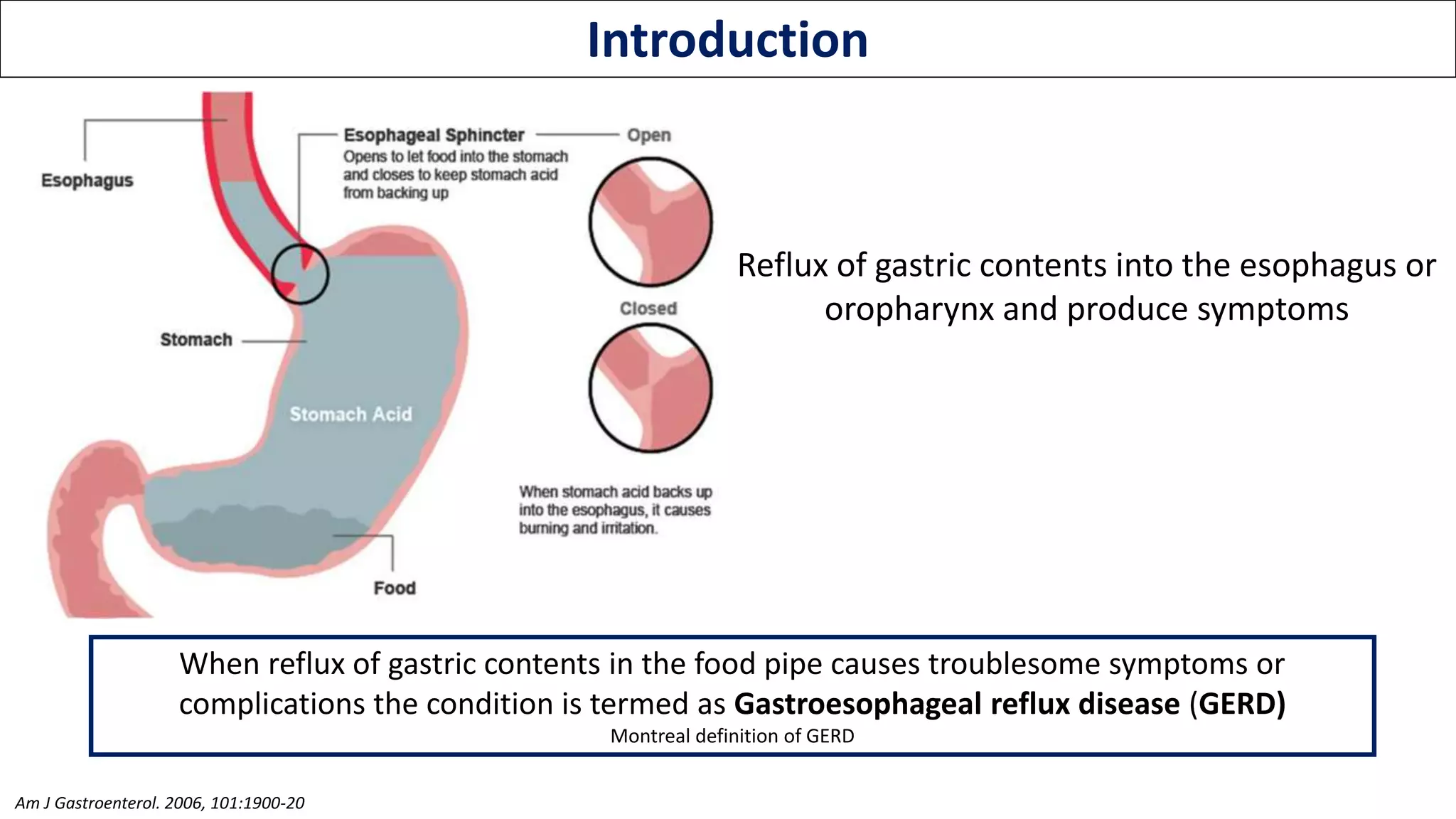
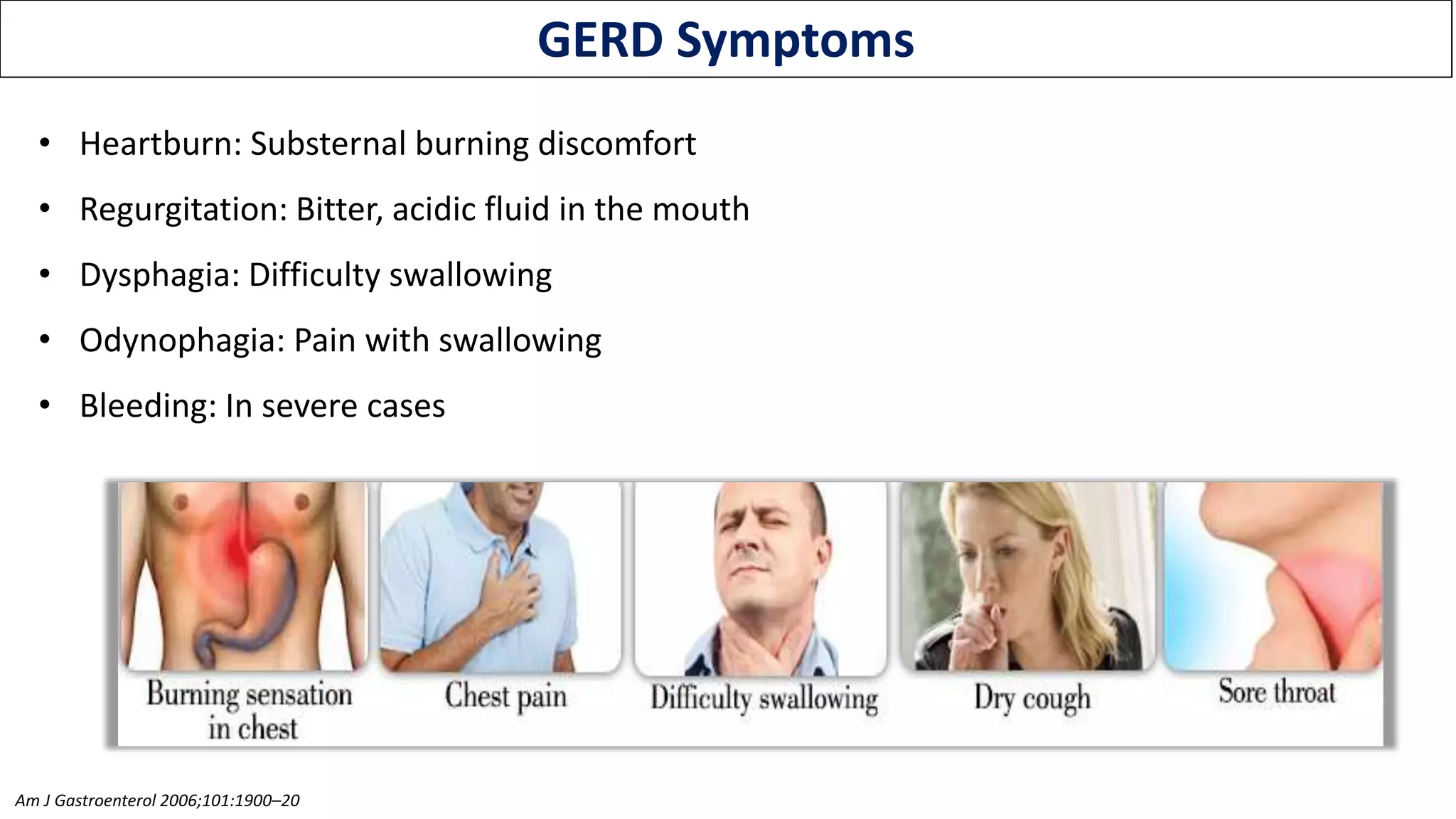
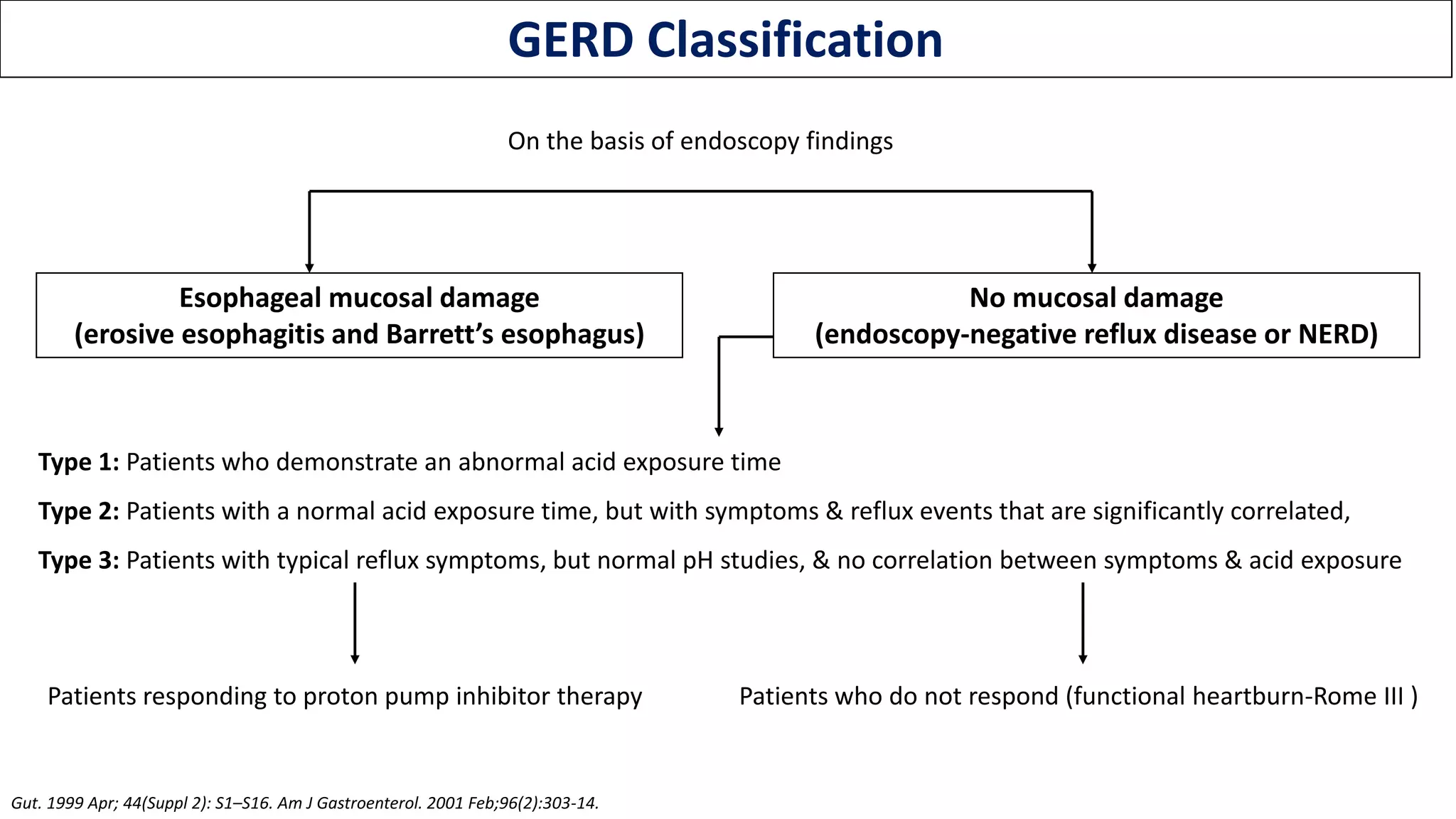
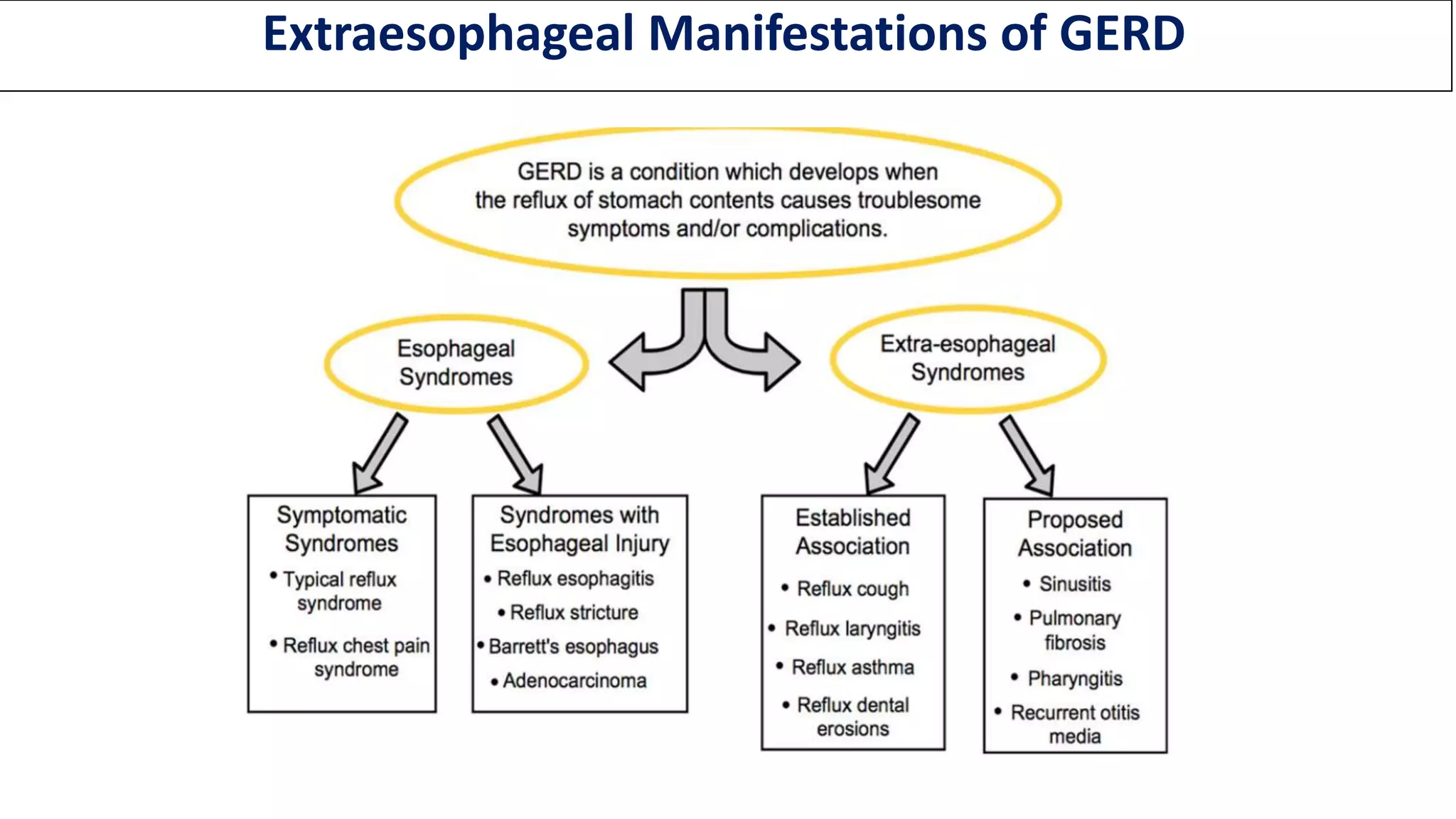
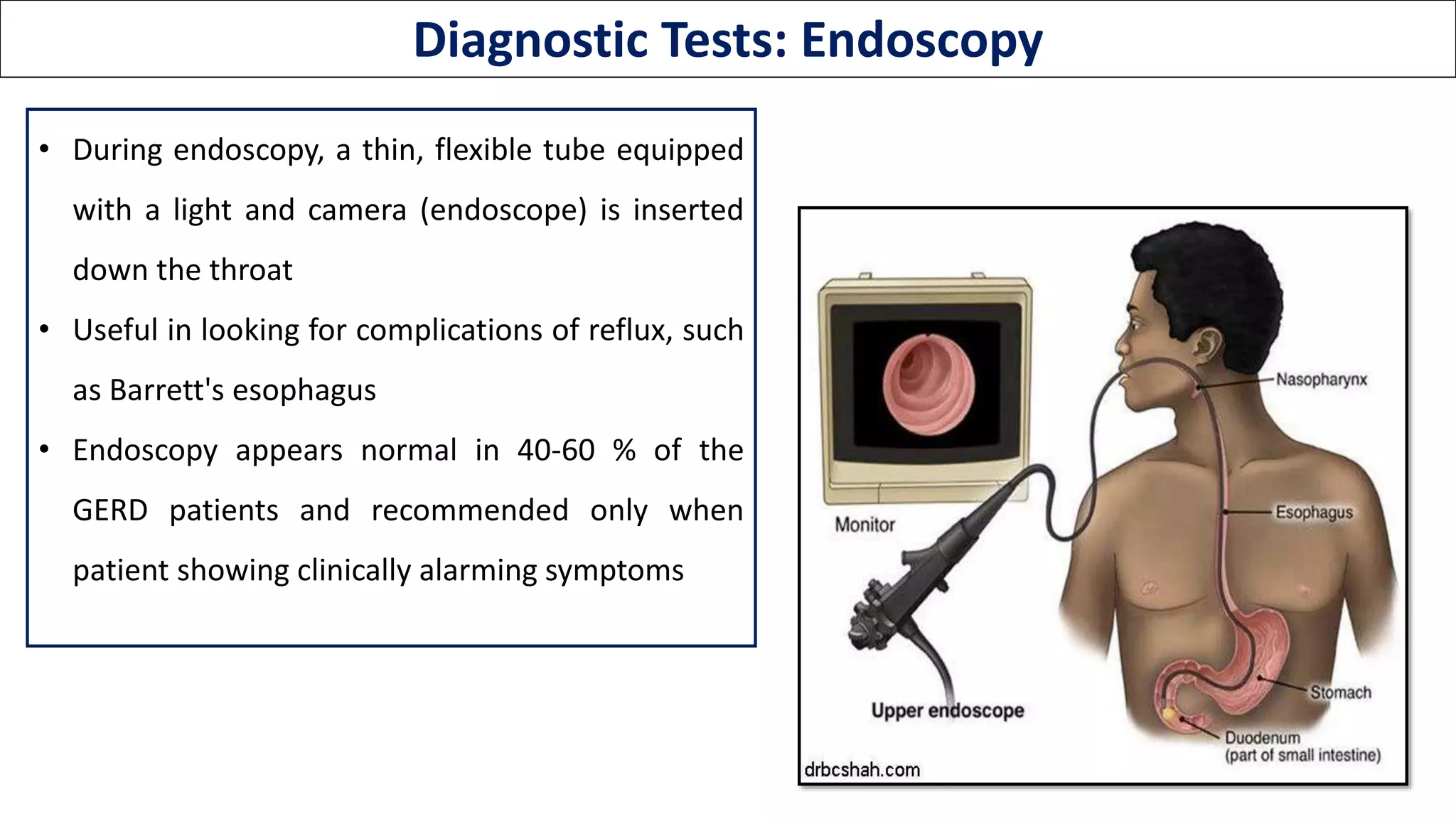
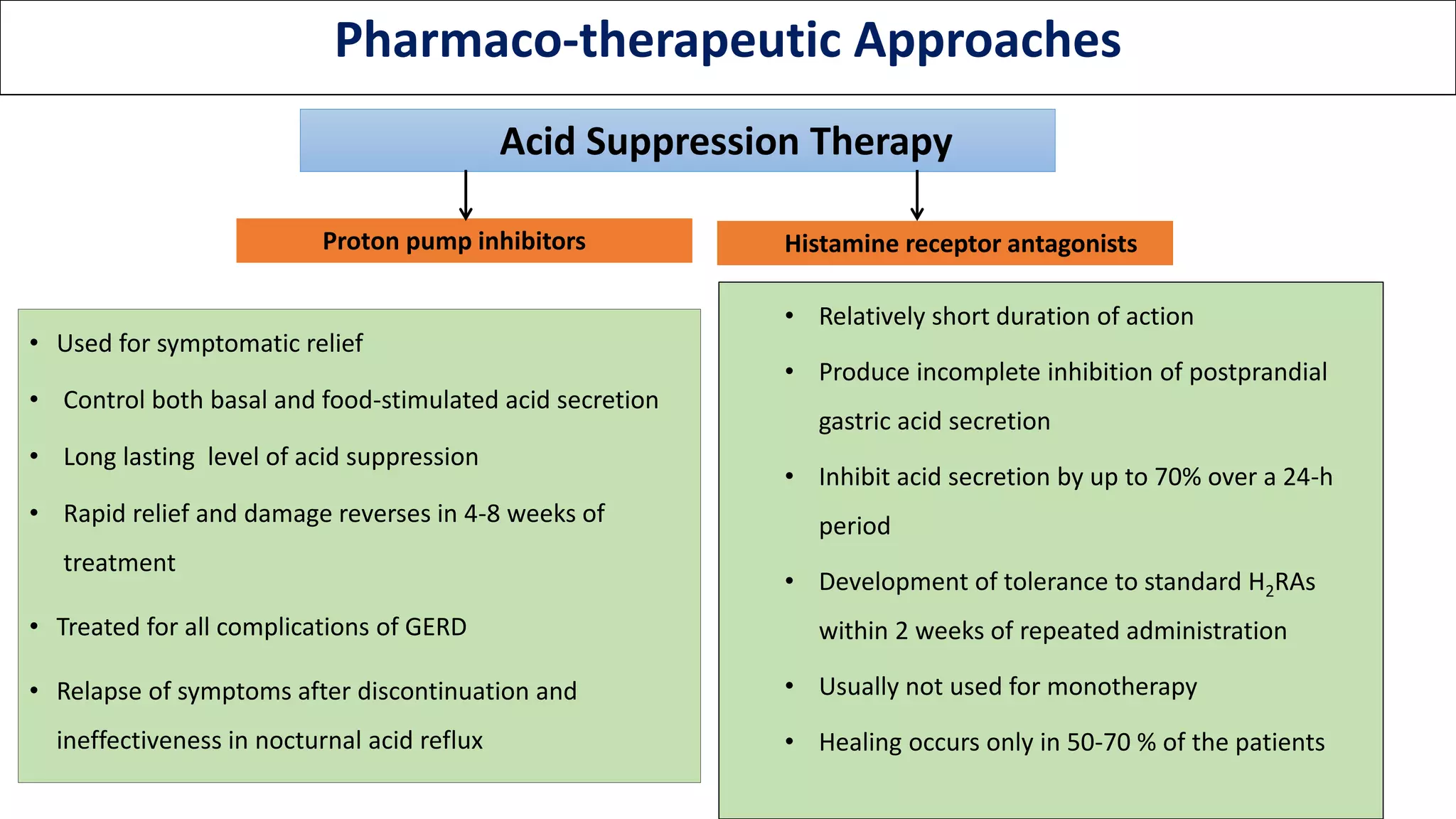
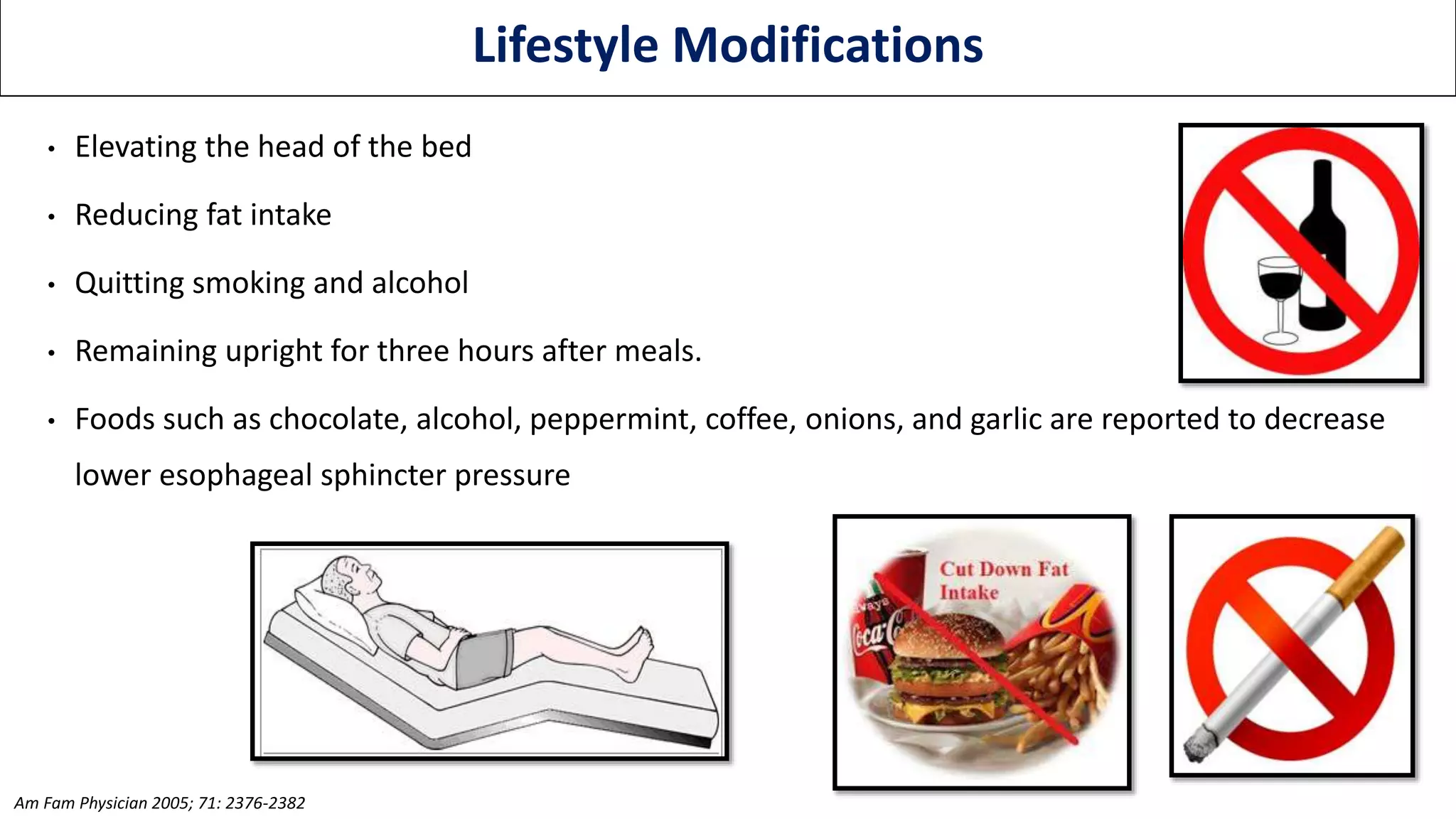
Gastroesophageal reflux disease (GERD) is caused by reflux of gastric contents into the esophagus, causing symptoms or complications. It affects 10-20% of the population in western countries. Symptoms include heartburn, regurgitation, dysphagia, and odynophagia. Diagnosis is usually made clinically but tests like endoscopy, pH monitoring, and manometry may be used. Treatment involves lifestyle modifications, medications like PPIs and H2 blockers, and sometimes surgery for severe or refractory cases. Proton pump inhibitors are very effective in relieving symptoms and healing esophagitis but need to be taken long-term. Surgery provides more durable treatment but