Downloaded 1,259 times
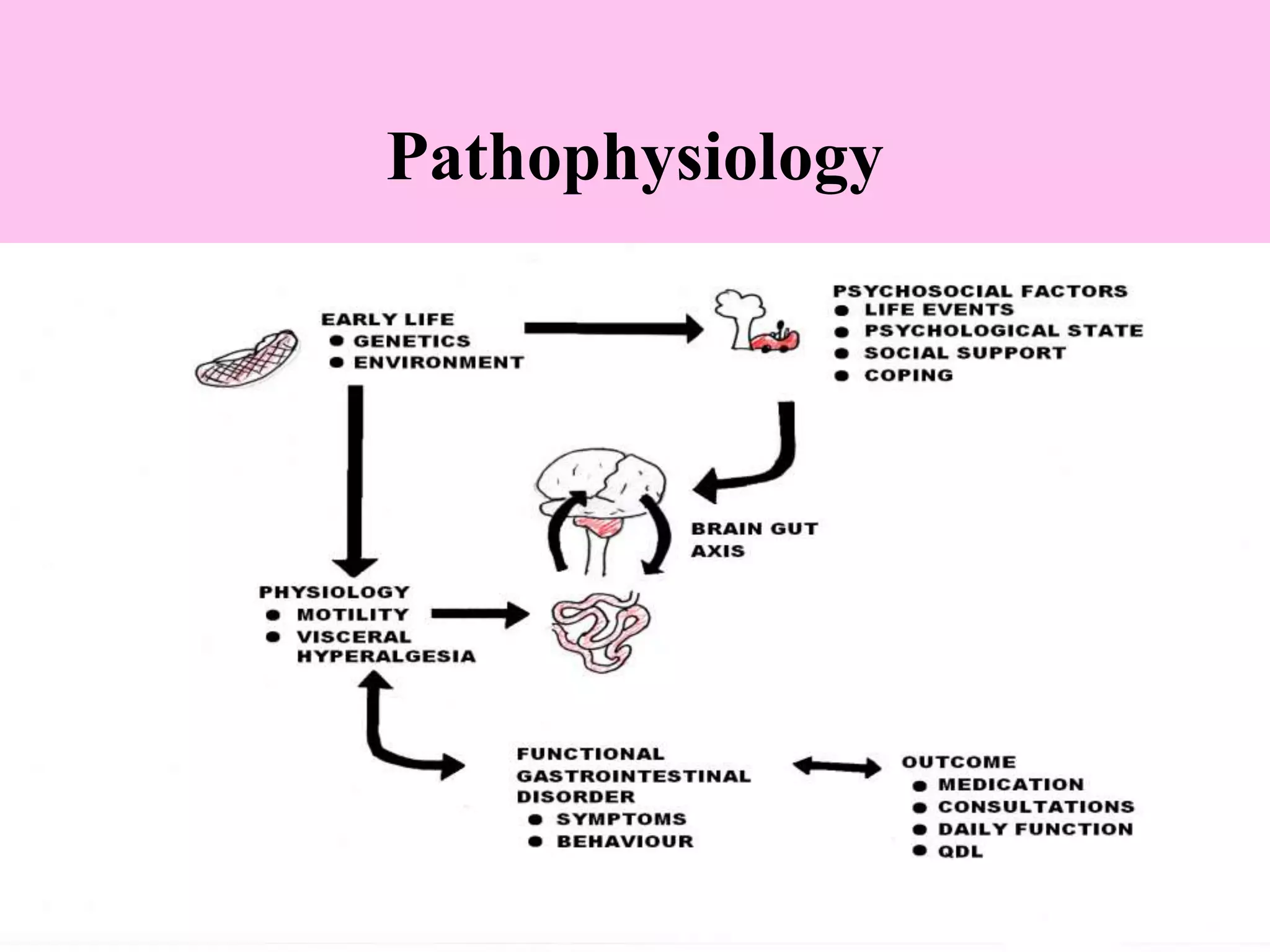
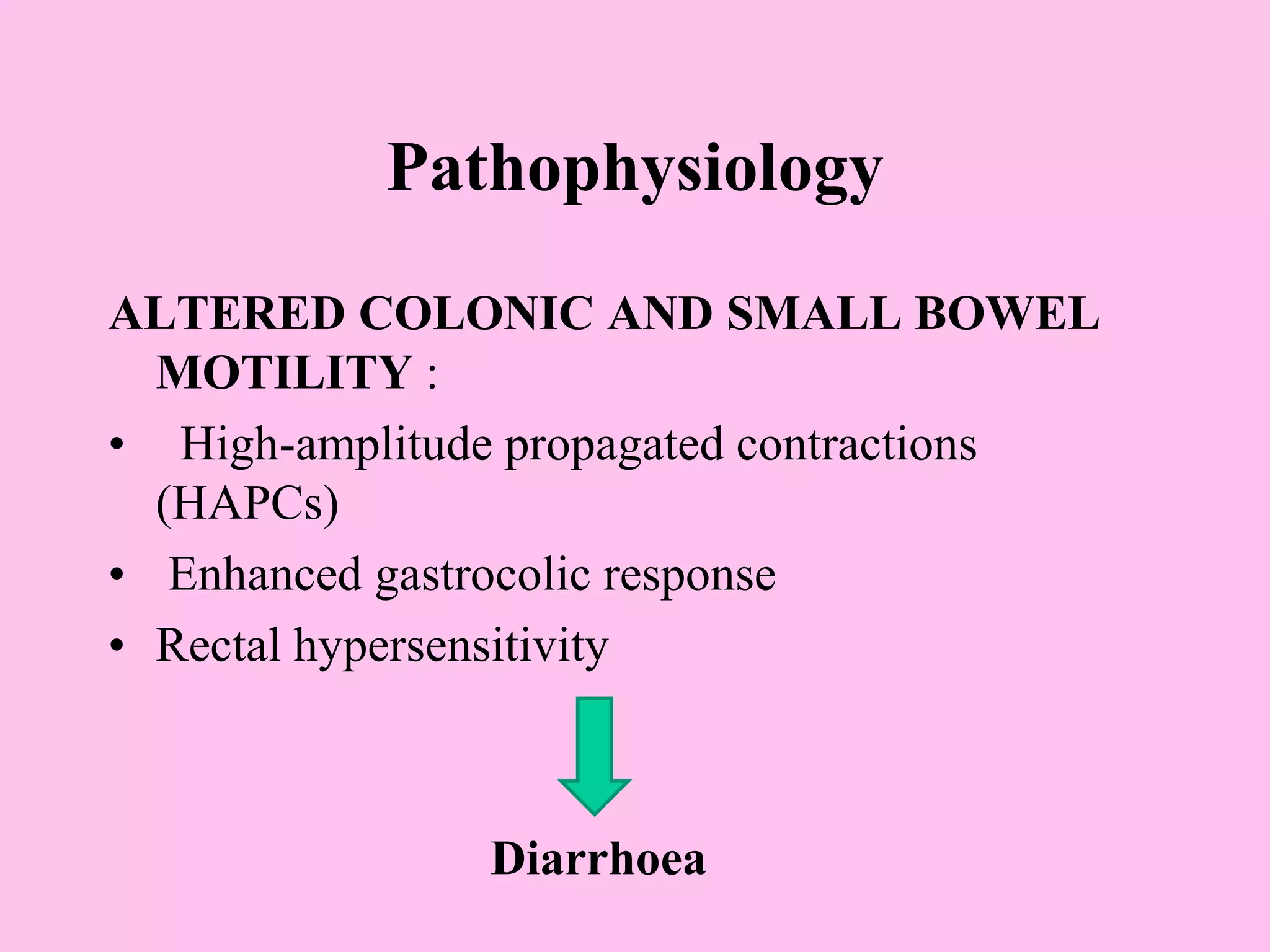
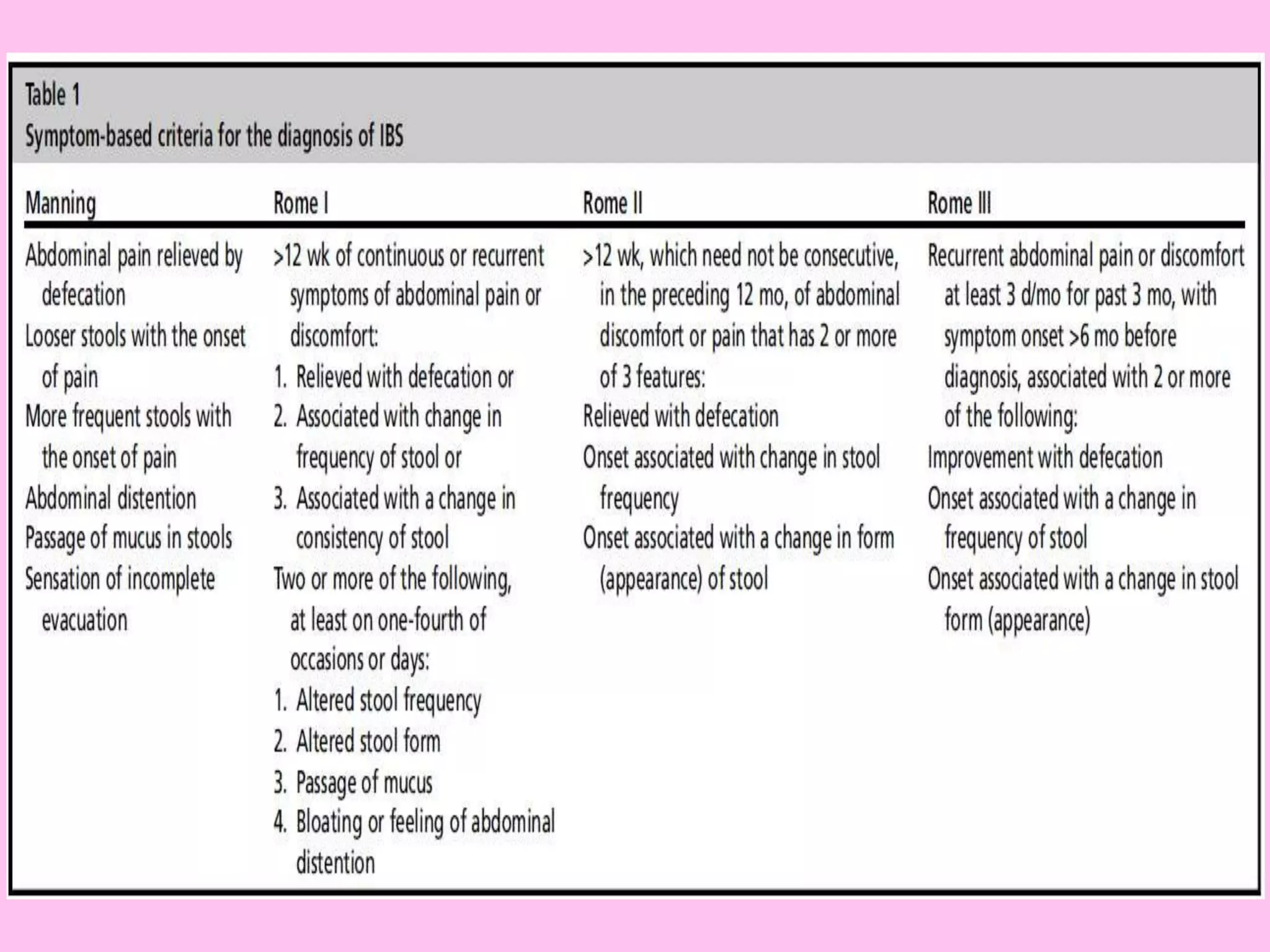
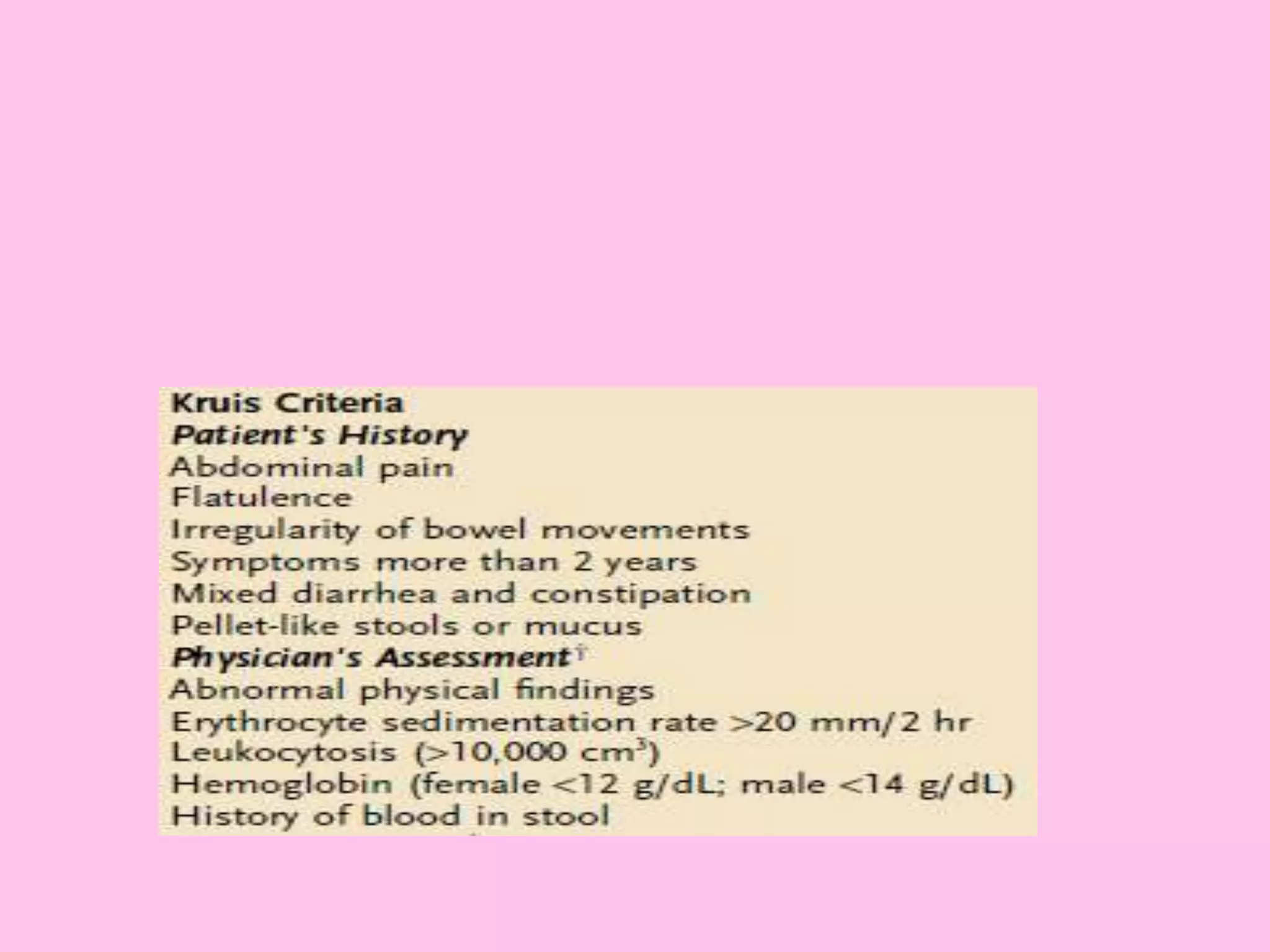
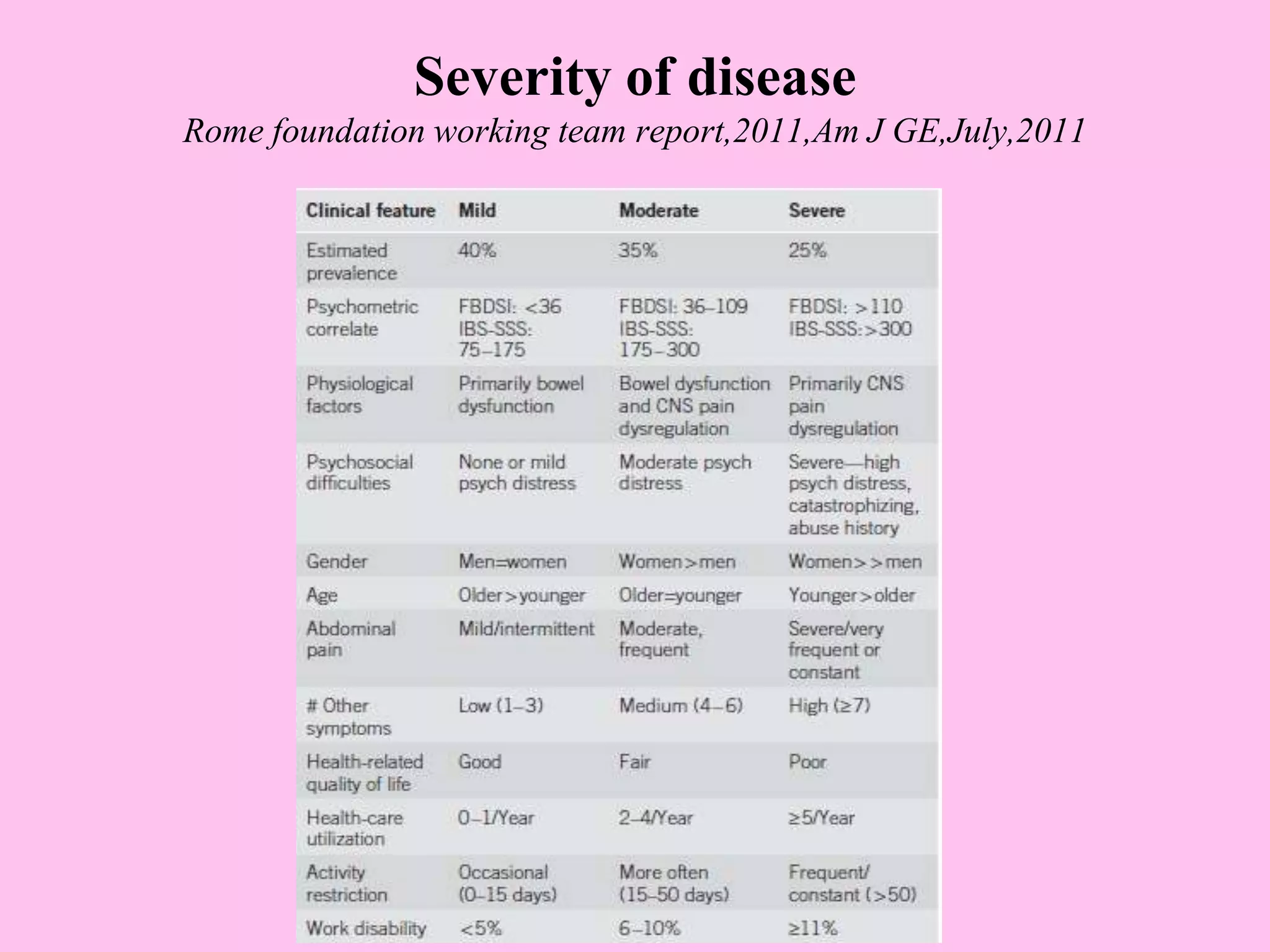
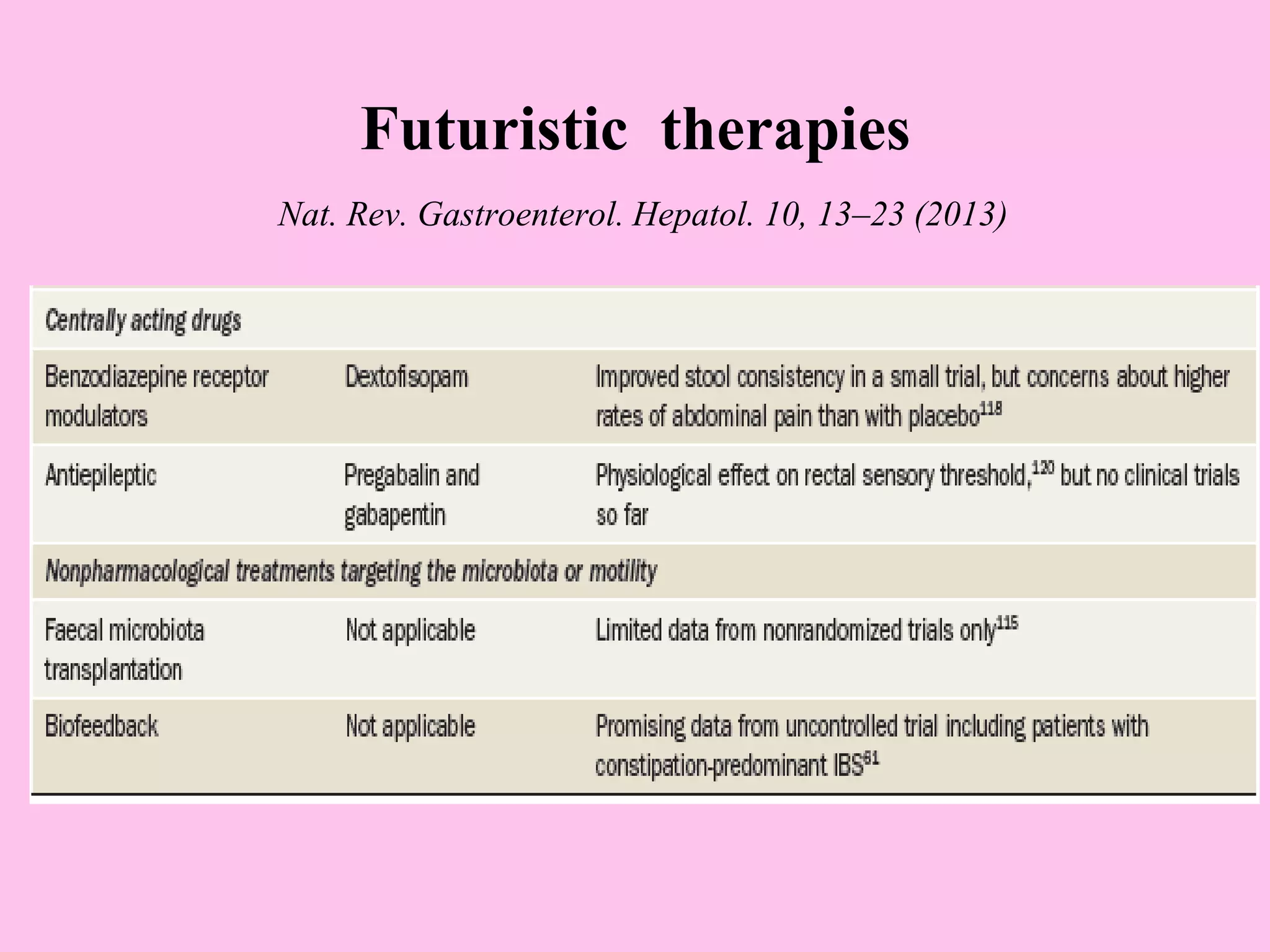


This document provides an overview of irritable bowel syndrome (IBS), including its definition, prevalence, demographics, pathophysiology, clinical features, diagnosis, differential diagnosis, severity assessment, management, and prognosis. Some key points are: - IBS is a functional bowel disorder characterized by abdominal pain associated with changes in bowel habits. It predominantly affects those aged 15-65 and is more common in women. - The pathophysiology involves altered gut motility, visceral hypersensitivity, abnormal gas handling, low-grade inflammation, food sensitivities, abnormal gut microbiota, and central nervous system dysregulation. - Diagnosis is based on symptoms meeting certain criteria and exclusion of organic diseases. Management focuses on




















































































