Downloaded 537 times




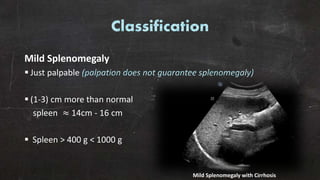









Splenomegaly is defined by enlarged splenic dimensions, typically categorized as mild, moderate, or massive based on size and weight. It can arise from various causes, including infections, cirrhosis, and other diseases, with associated symptoms such as fever and abdominal pain. Diagnosis involves imaging techniques and blood tests, with severe cases possibly leading to splenectomy.





























![[Int. med] spleenomegaly from SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/vcnwsy2ltcejz2qexiuf-signature-b01672da1ecf8b94befb115319b147a085de390b8cb403389bce6c156545fbb5-poli-150815171704-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)

















































