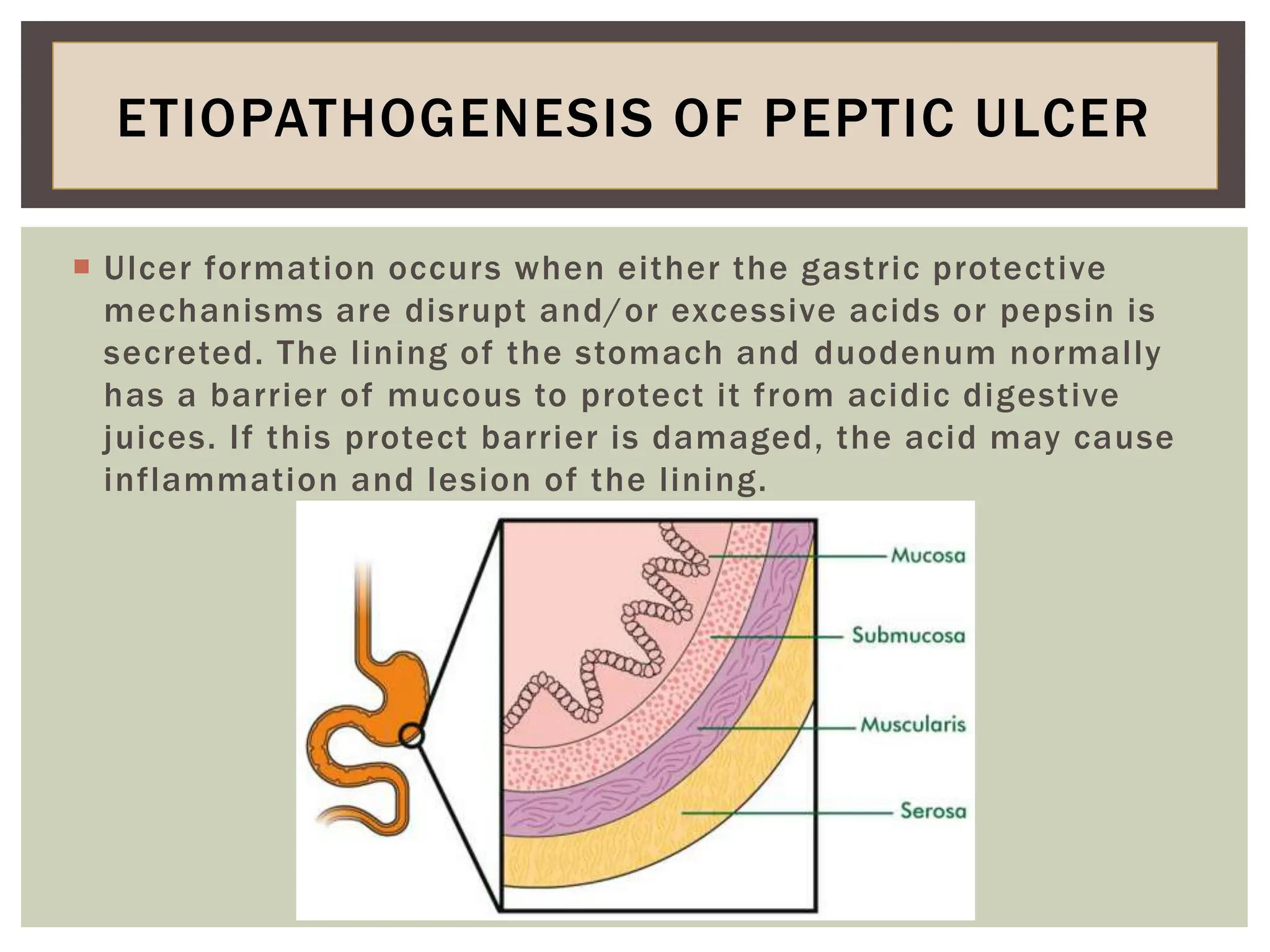
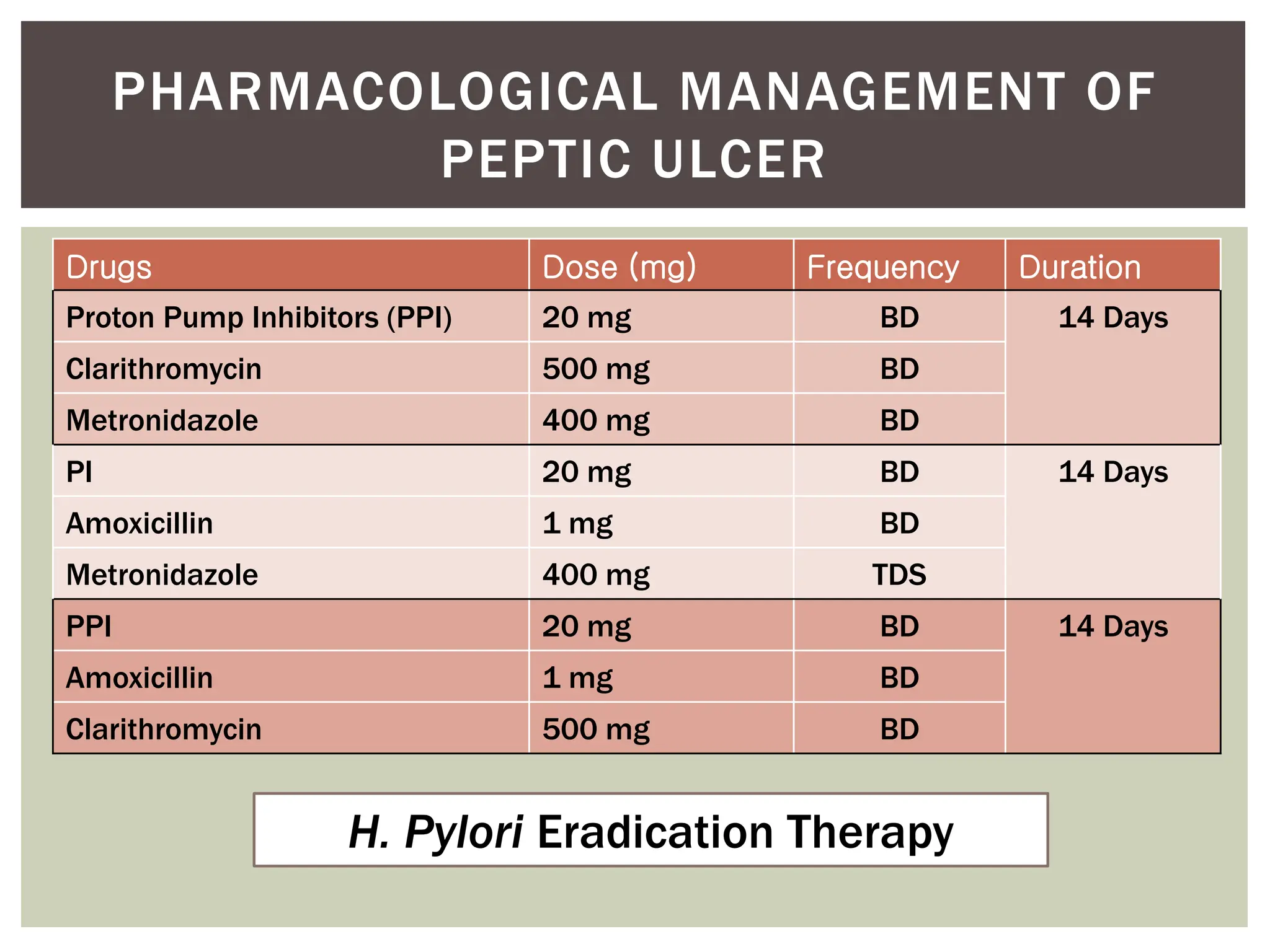
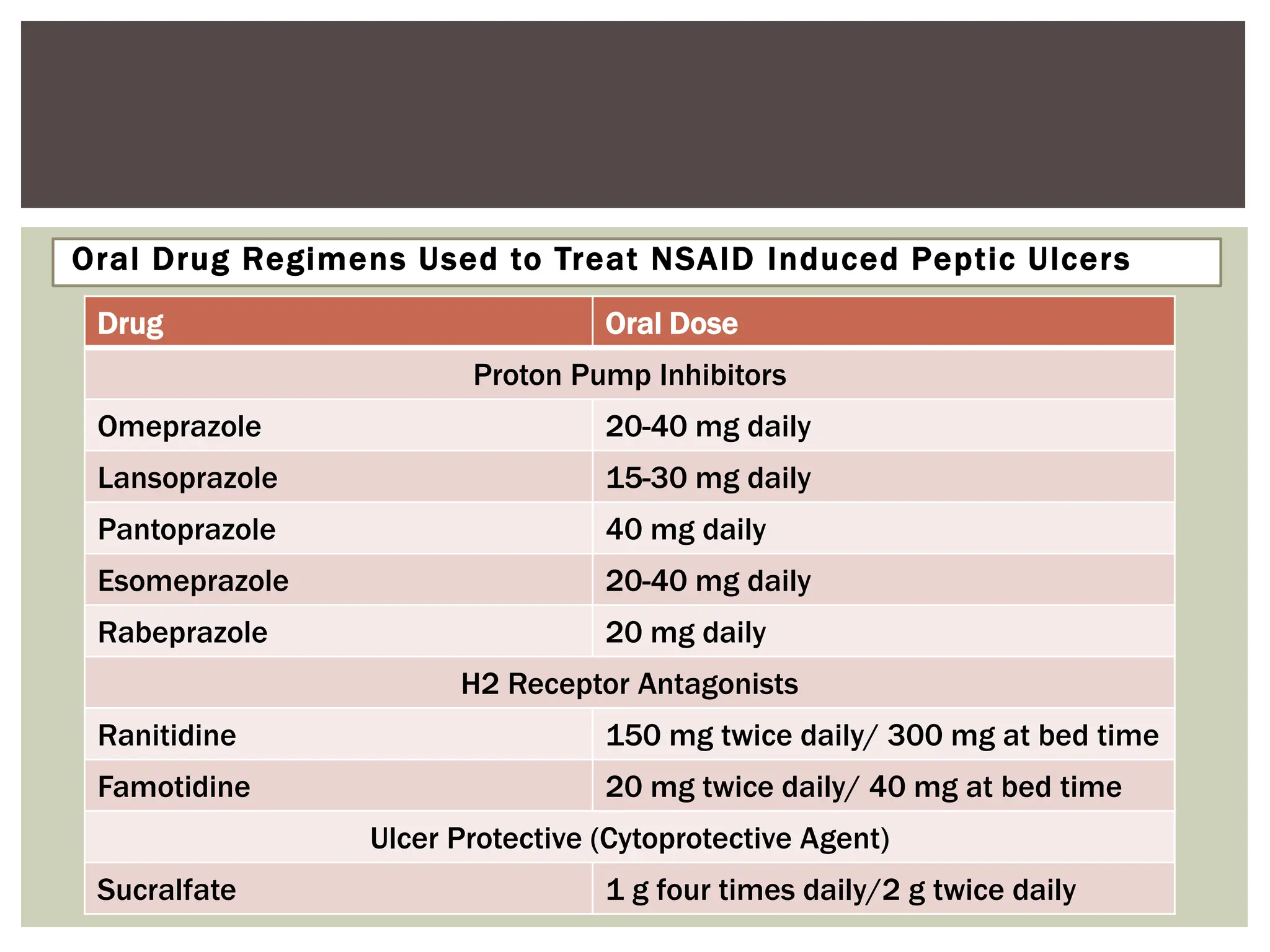
The document provides a comprehensive overview of gastrointestinal disorders, focusing on gastroesophageal reflux disease (GERD), peptic ulcer disease (PUD), alcoholic liver disease (ALD), and inflammatory bowel diseases like Crohn's disease and ulcerative colitis. It details the pathophysiology, risk factors, clinical manifestations, diagnostic approaches, and management options for each condition. Treatment strategies discussed include lifestyle modifications, pharmacological therapies, and surgical interventions as indicated for complications.