Downloaded 2,572 times

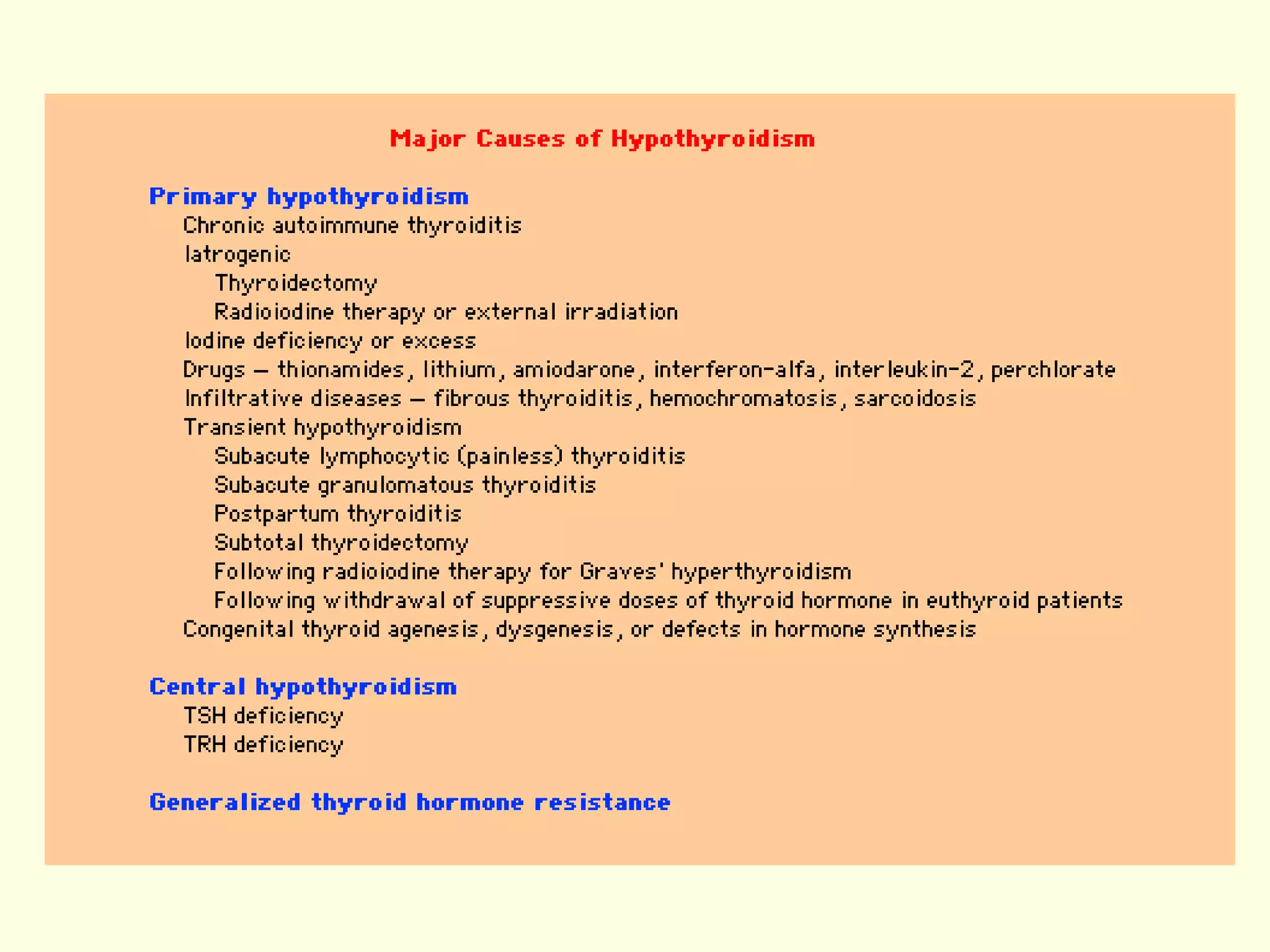







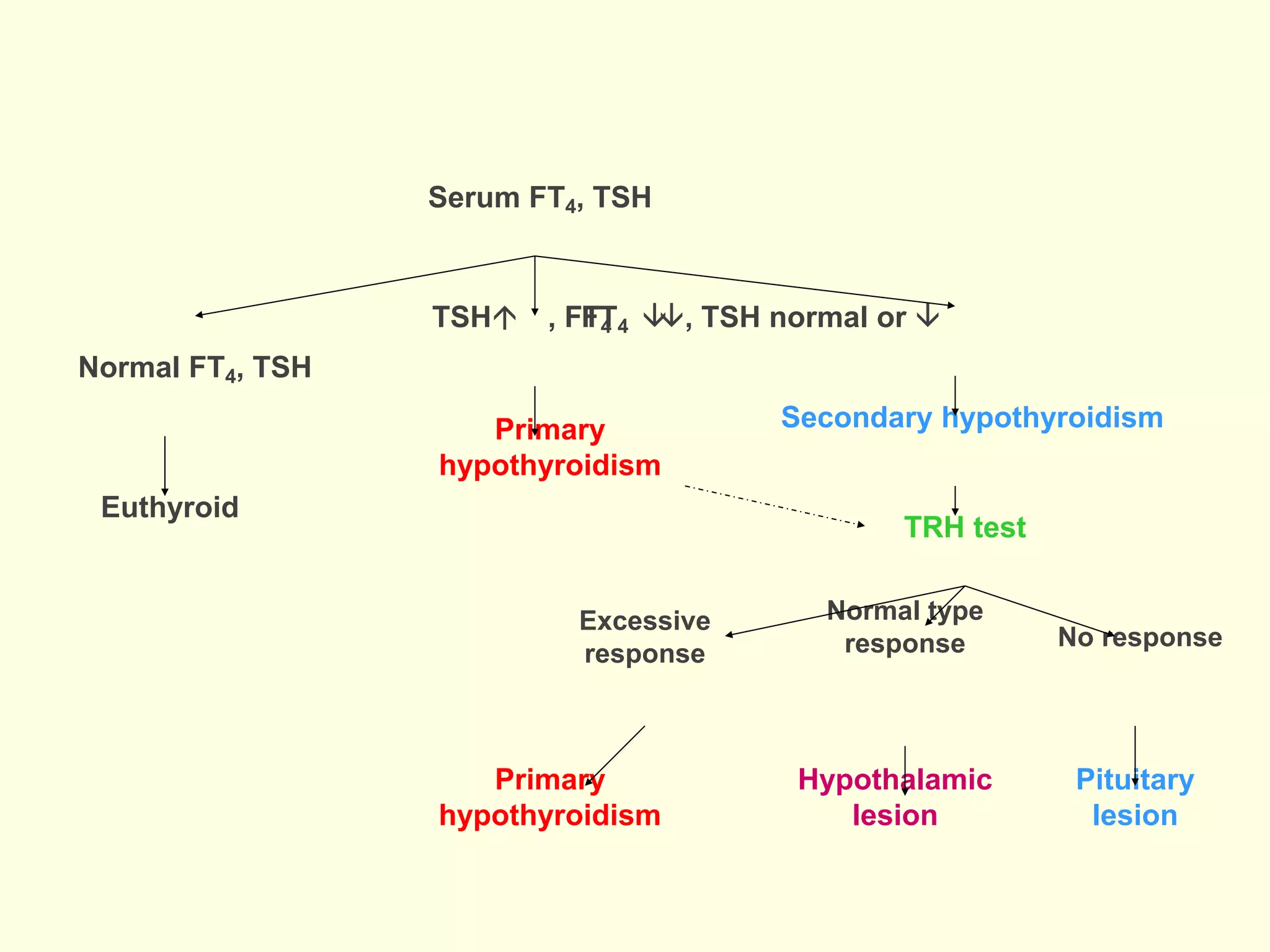




Hypothyroidism is a clinical syndrome caused by a deficiency of thyroid hormones, leading to a generalized slowing of metabolic processes, with various symptoms across different age groups. The condition can stem from primary thyroid failure, secondary pituitary issues, or less commonly, tertiary hypothalamic deficiencies, with Hashimoto's thyroiditis being the most common cause. Treatment involves levothyroxine (T4) replacement therapy, with dosage adjustments as needed based on patient age and physiological conditions.







































































































