Downloaded 1,242 times
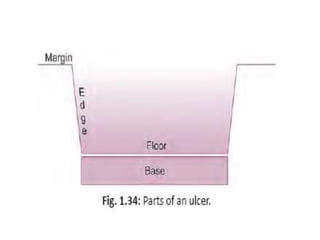
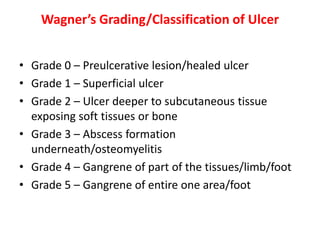
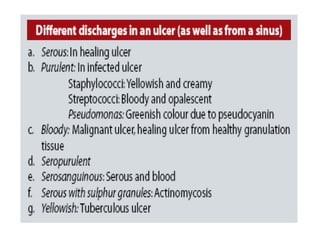
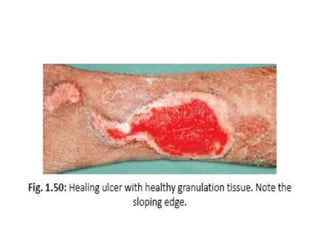
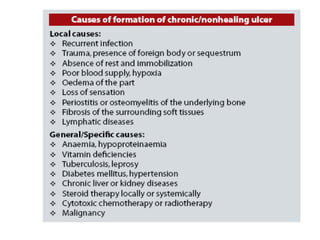


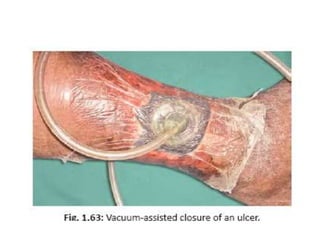












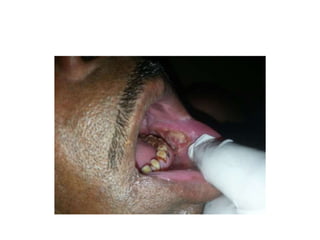

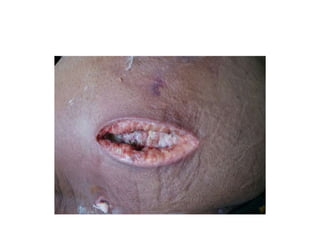


This document discusses ulcers, including their definition, parts, classifications, investigations, and management. It defines an ulcer as a break in the skin or mucous membrane epithelium due to cell death. The key parts of an ulcer are the margin, edge, floor, and base. Ulcers can be classified clinically based on healing status, duration, or etiology. Investigations may include wound cultures, biopsies, and imaging. Management involves treating the underlying cause, wound cleaning, debridement, dressings, and therapies like vacuum-assisted closure or maggot debridement to promote healing.



















































































