Downloaded 392 times
![PUD TREATMENT
1. Antacids eg. Mylanta, Maalox, Tums, Gaviscon (100-140 meq/L 1 and 3 h after
meals )
2. Triple therapy is the first line treatment - PPI taken simultaneously with two
antibiotics (from amoxicillin, clarithromycin and metronidazole) for 7 or 14 days.
3. 10-14 days of bismuth quadruple therapy(bismuth, proton pump inhibitor [PPI],
tetracycline, and a nitroimidazole).
4. Surgical interventions.](https://image.slidesharecdn.com/zollingerellisonsyndrome-170412163413/85/Zollinger-ellison-syndrome-14-320.jpg)

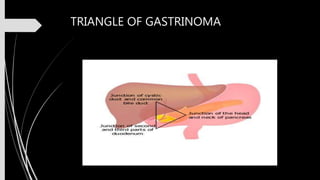
This document discusses Zollinger-Ellison syndrome, which is characterized by severe peptic ulcers caused by excessive stomach acid production due to a non-beta cell tumor known as a gastrinoma. It describes the pathophysiology, tumor distribution, clinical manifestations, diagnosis, and treatment of the condition. The gastrinoma secretes gastrin which stimulates acid secretion, potentially reaching the small intestine and inactivating pancreatic enzymes. Diagnosis involves biochemical tests and imaging to locate the tumor. Treatment options include proton pump inhibitors, somatostatin analogues, and surgery to cure the condition.






































































































