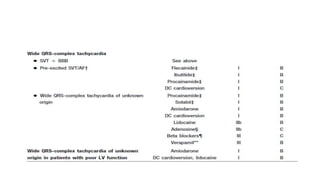
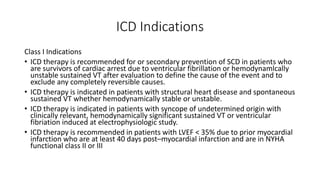
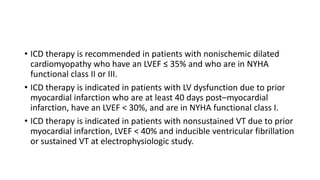
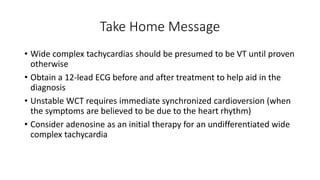
Wide complex tachycardia refers to a cardiac rhythm with a rate over 100 beats per minute and a QRS duration of 120 ms or more. It can be caused by ventricular tachycardia originating in the ventricles, or supraventricular tachycardia with aberrancy or pre-excitation. Differentiating the two is important as treatment differs. The electrocardiogram and various diagnostic criteria and algorithms using features like QRS duration, axis, and morphology can help determine the origin of the arrhythmia. Treatment involves terminating unstable rhythms with cardioversion or medications, while implanting defibrillators may help prevent recurrence in some patients.
![• Widening of the QRS complex is related to slower spread of ventricular
depolarization, either due to disease of the His-Purkinje network and/or reliance
on slower, muscle-to-muscle spread of depolarization.
1. propagation of a supraventricular impulse (atrial premature depolarizations
[APDs] or supraventricular tachycardia [SVT]) with block (preexisting or rate-
related) in one or more parts of the His-Purkinje network;
2. depolarizations originating in the ventricles themselves (ventricular premature
beats [VPDs] or ventricular tachycardia [VT]);
3. slowed propagation of a supraventricular impulse because of intra-myocardial
scar/fibrosis/hypertrophy; or
4. conduction of a supraventricular impulse from atrium to ventricle over an
accessory pathway (bypass tract) – so called “pre-excited” tachycardia.](https://image.slidesharecdn.com/widecomplextachycardia-180415151603/85/Wide-complex-tachycardia-3-320.jpg)