

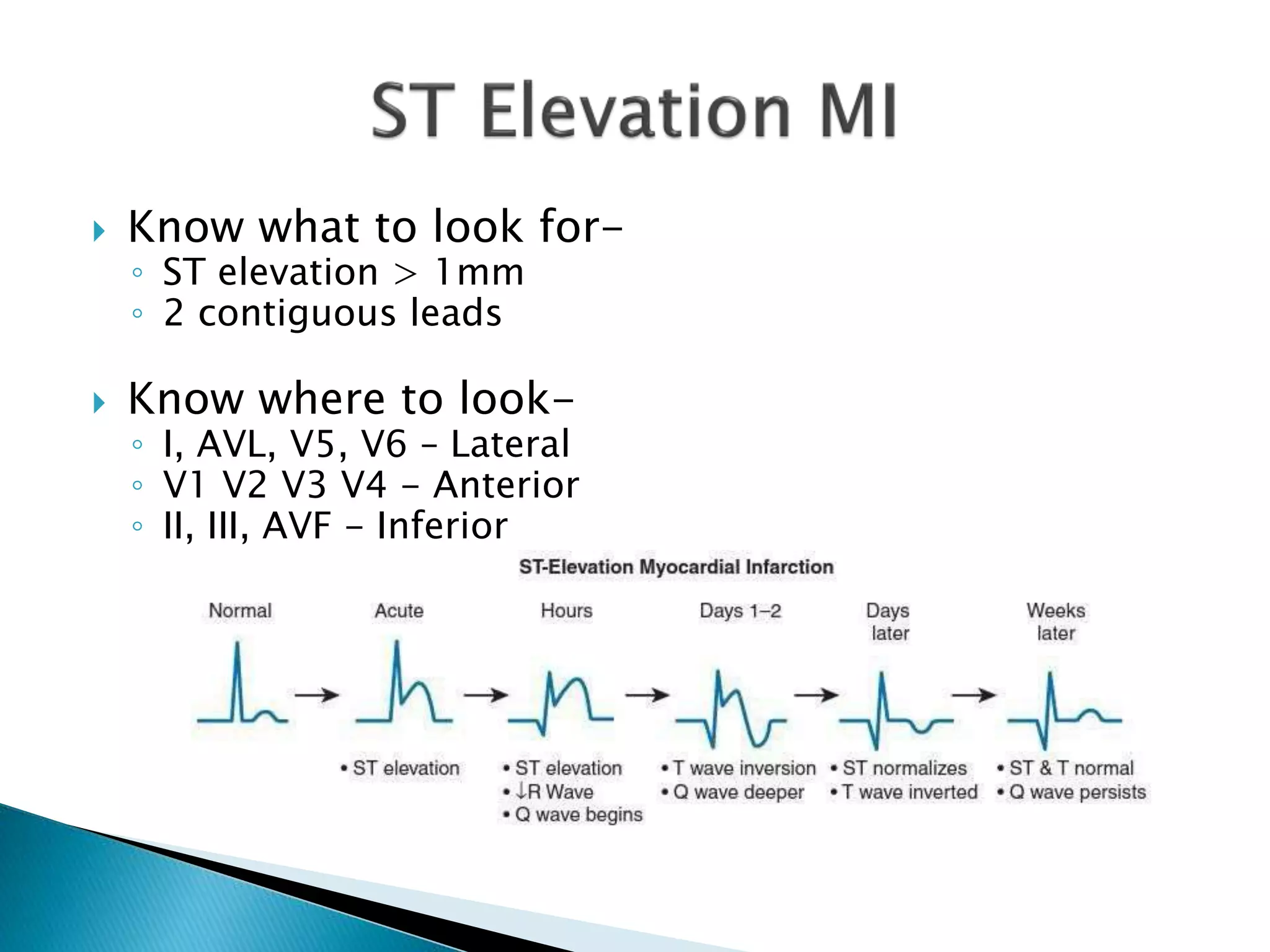

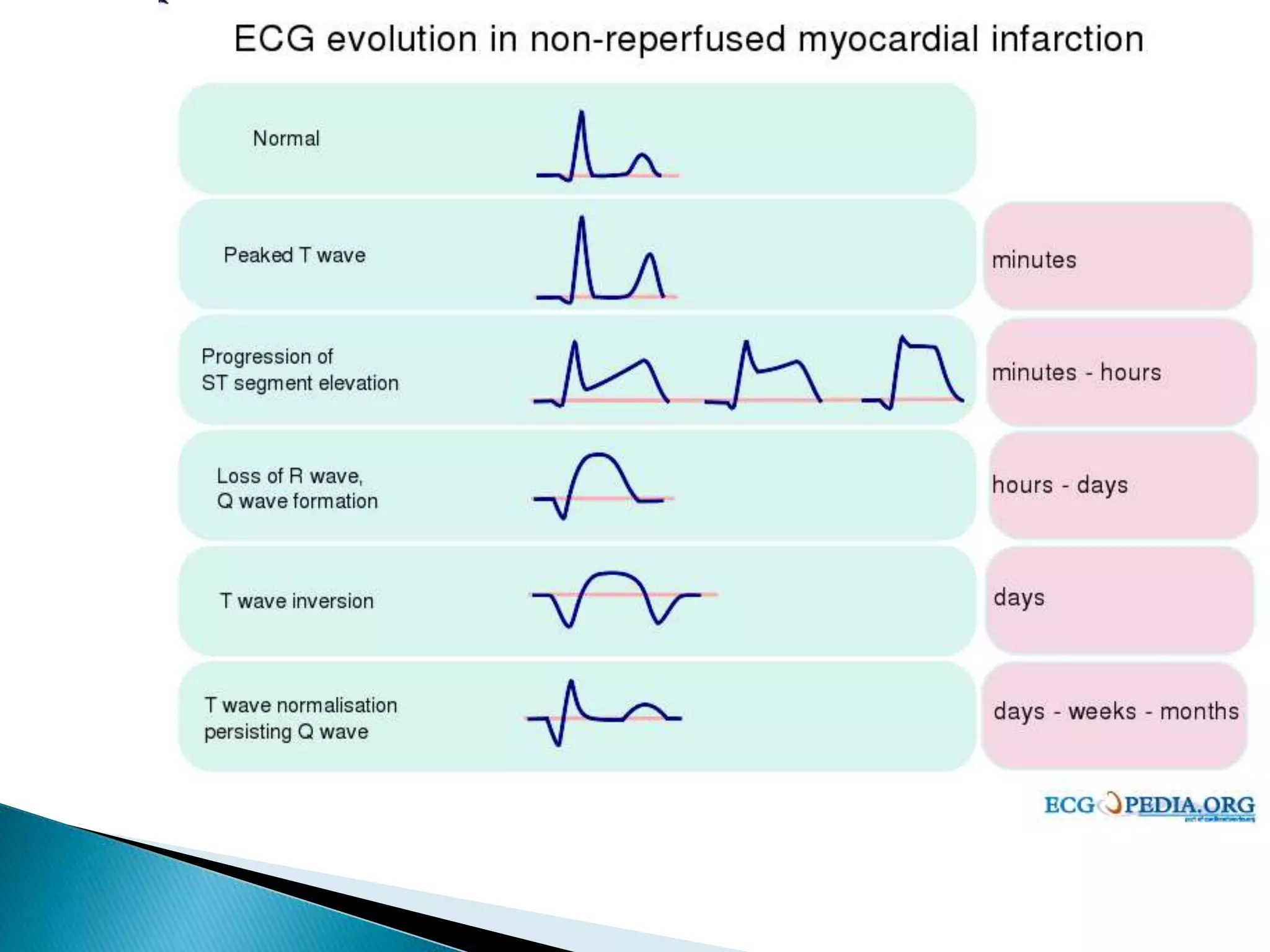
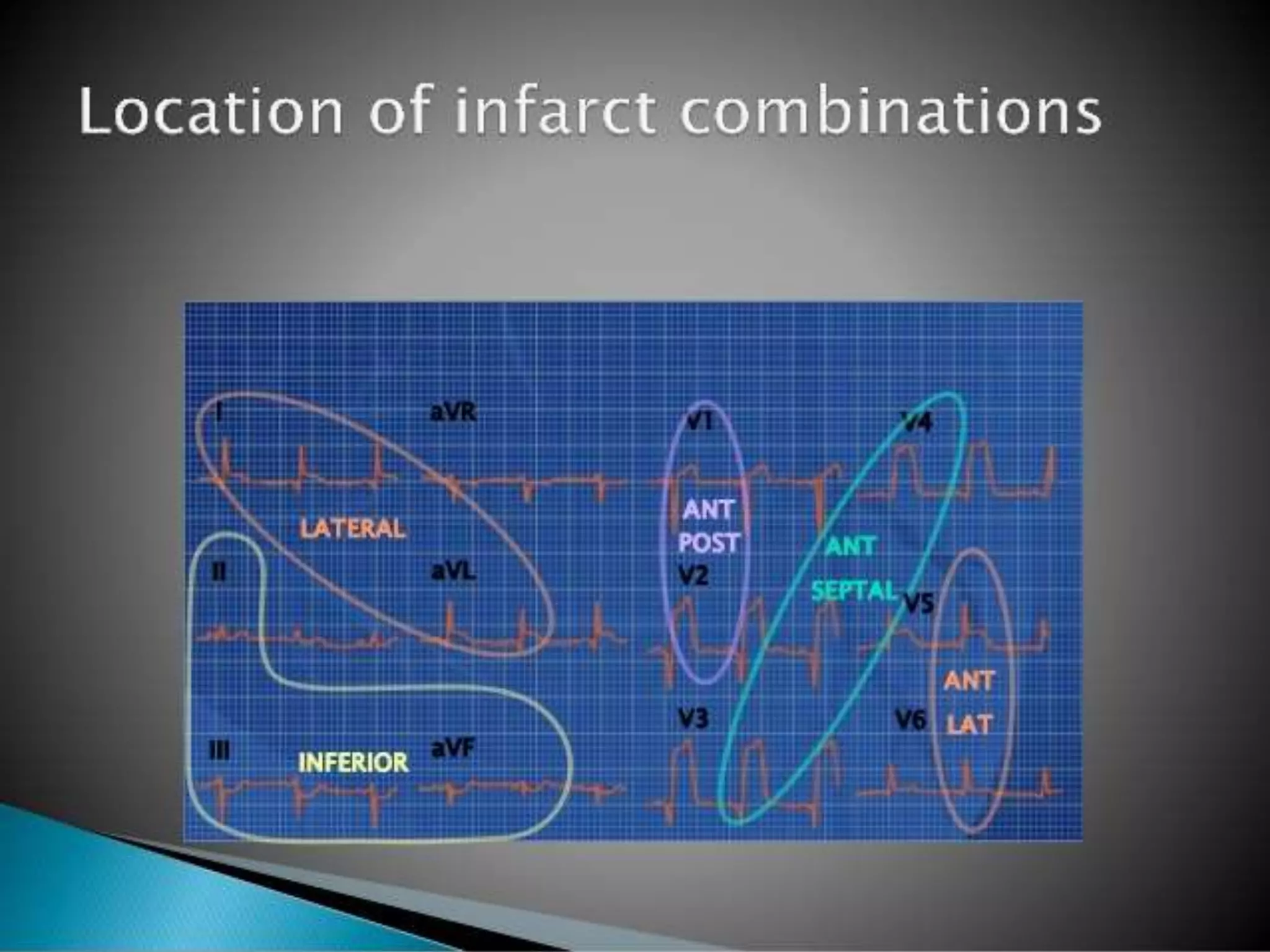
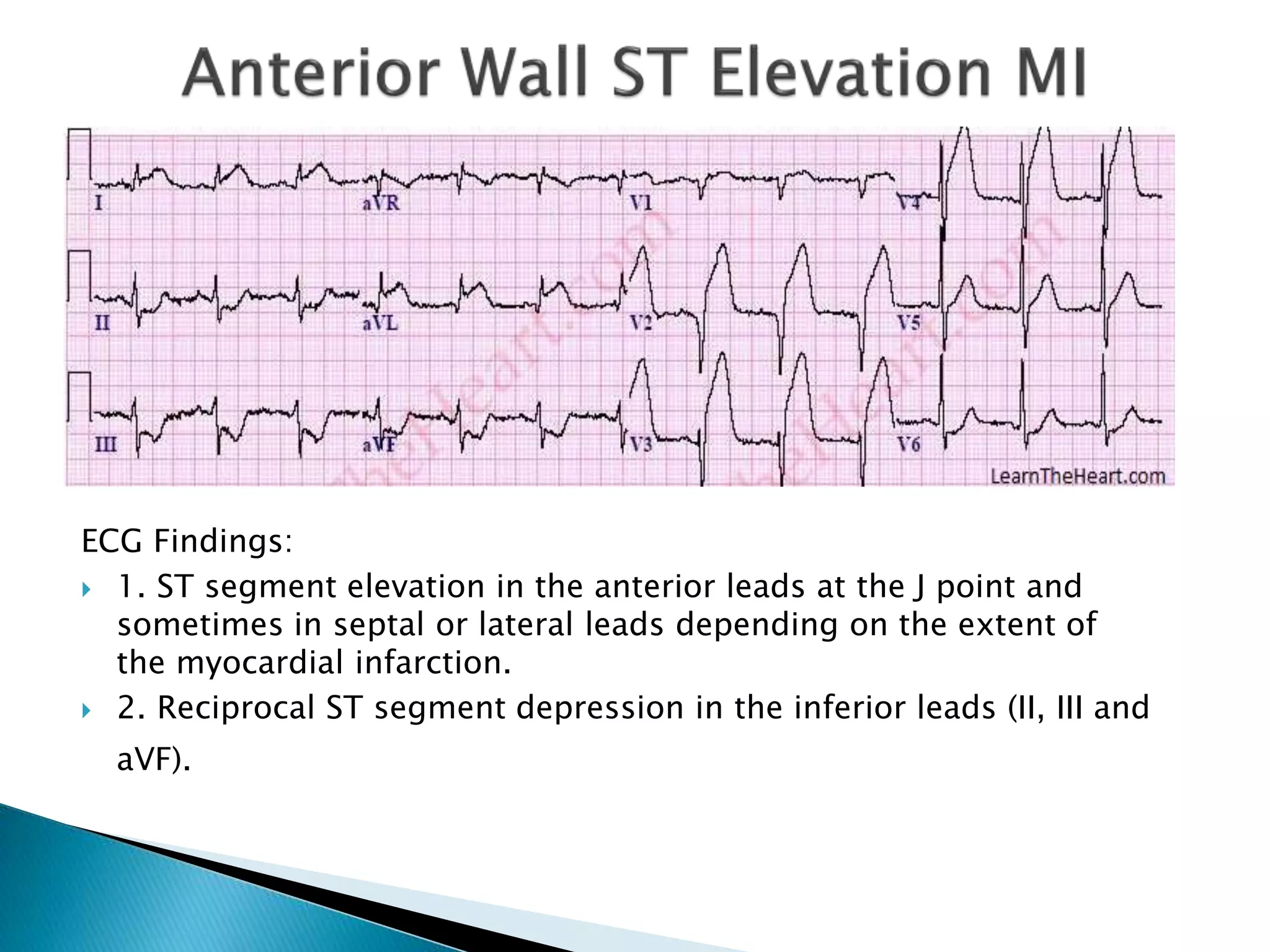

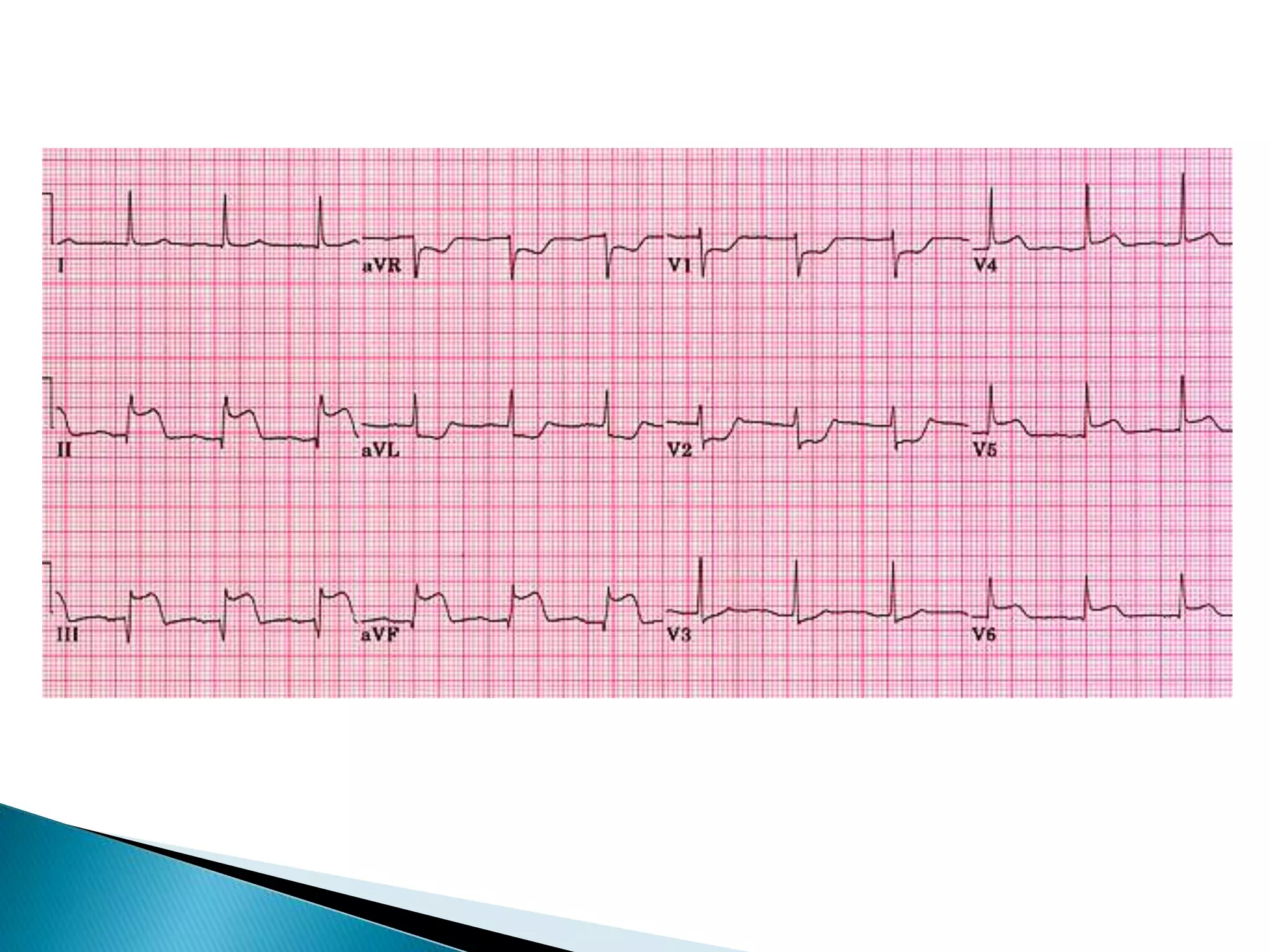

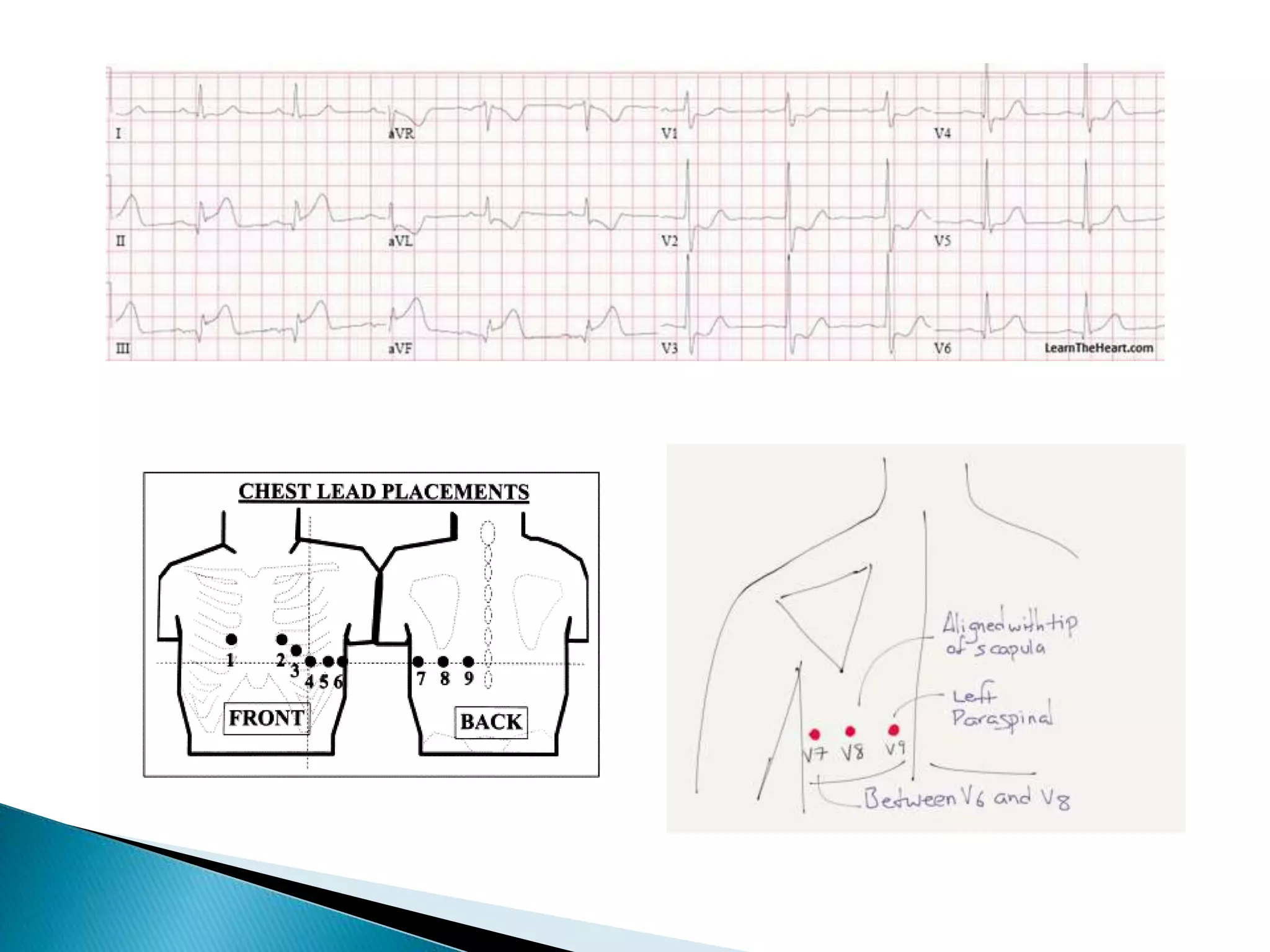




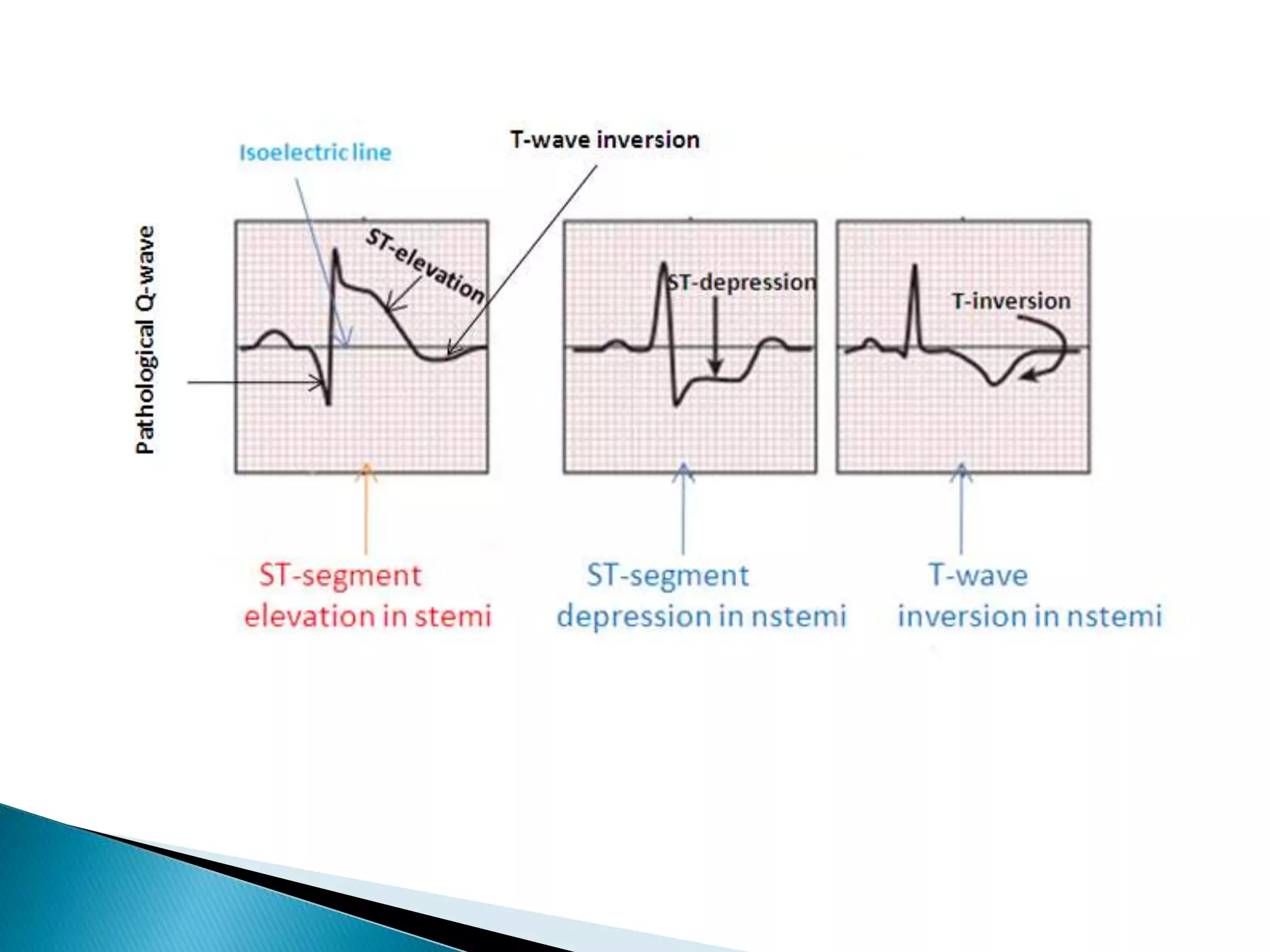
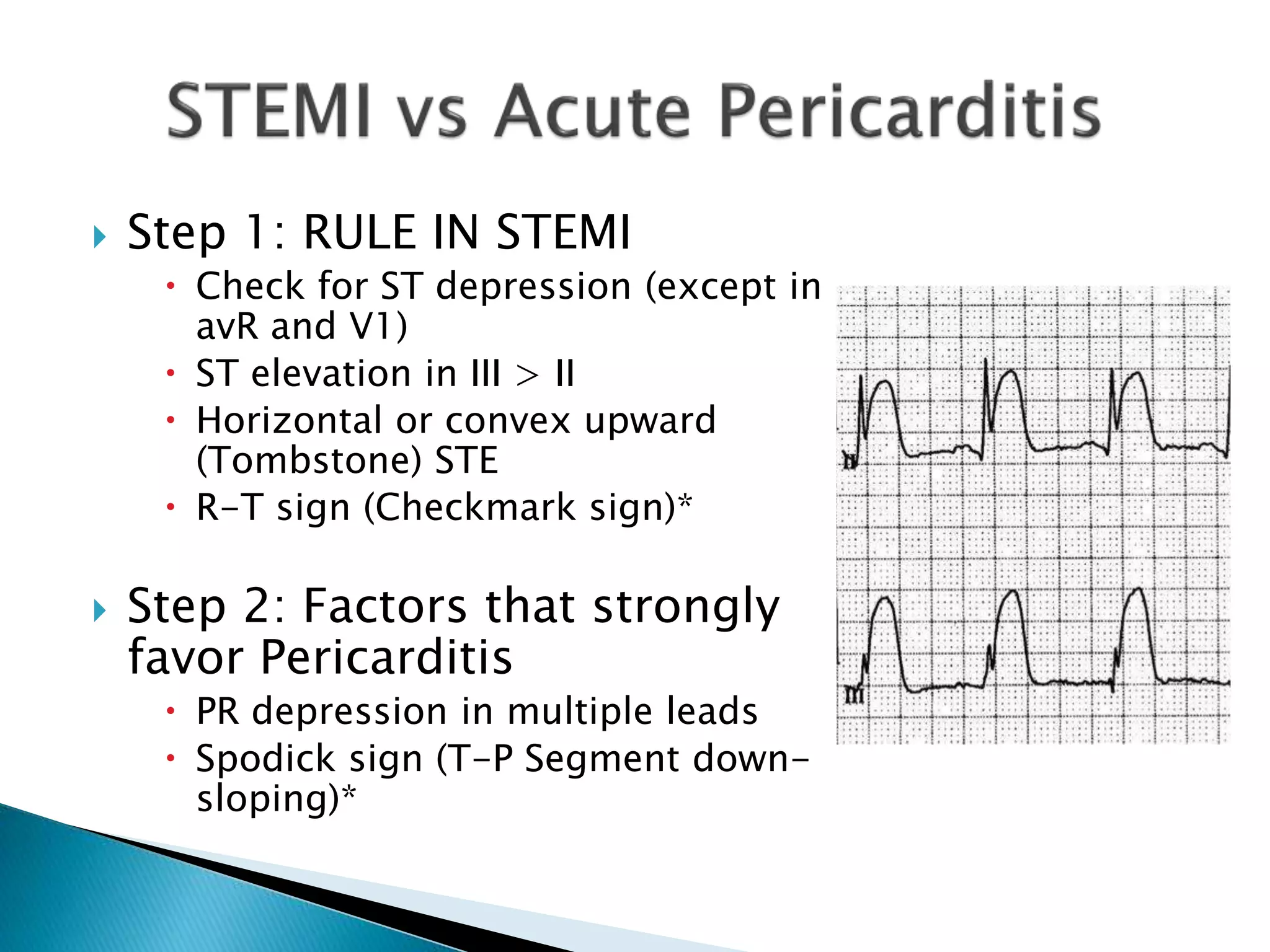
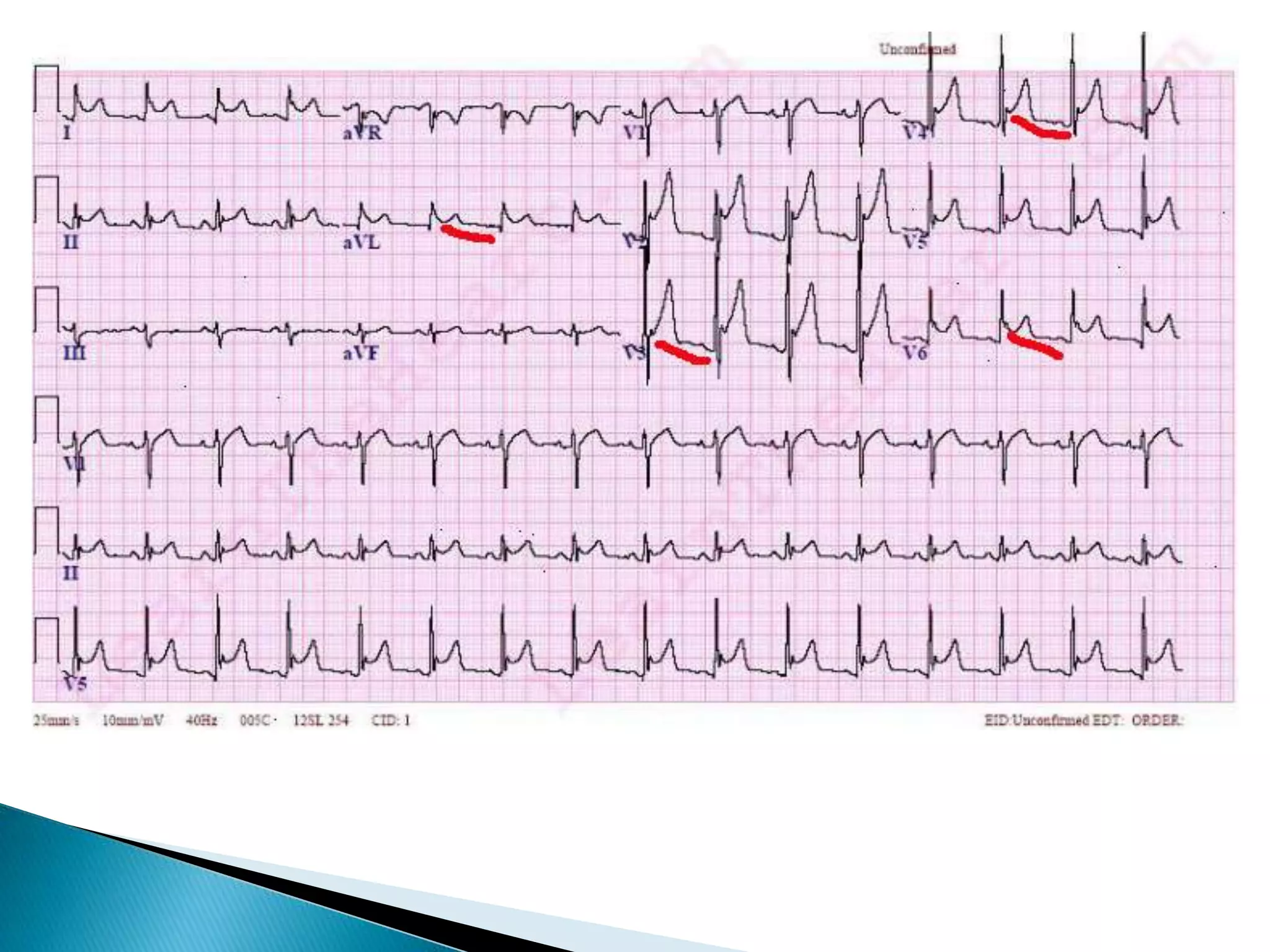

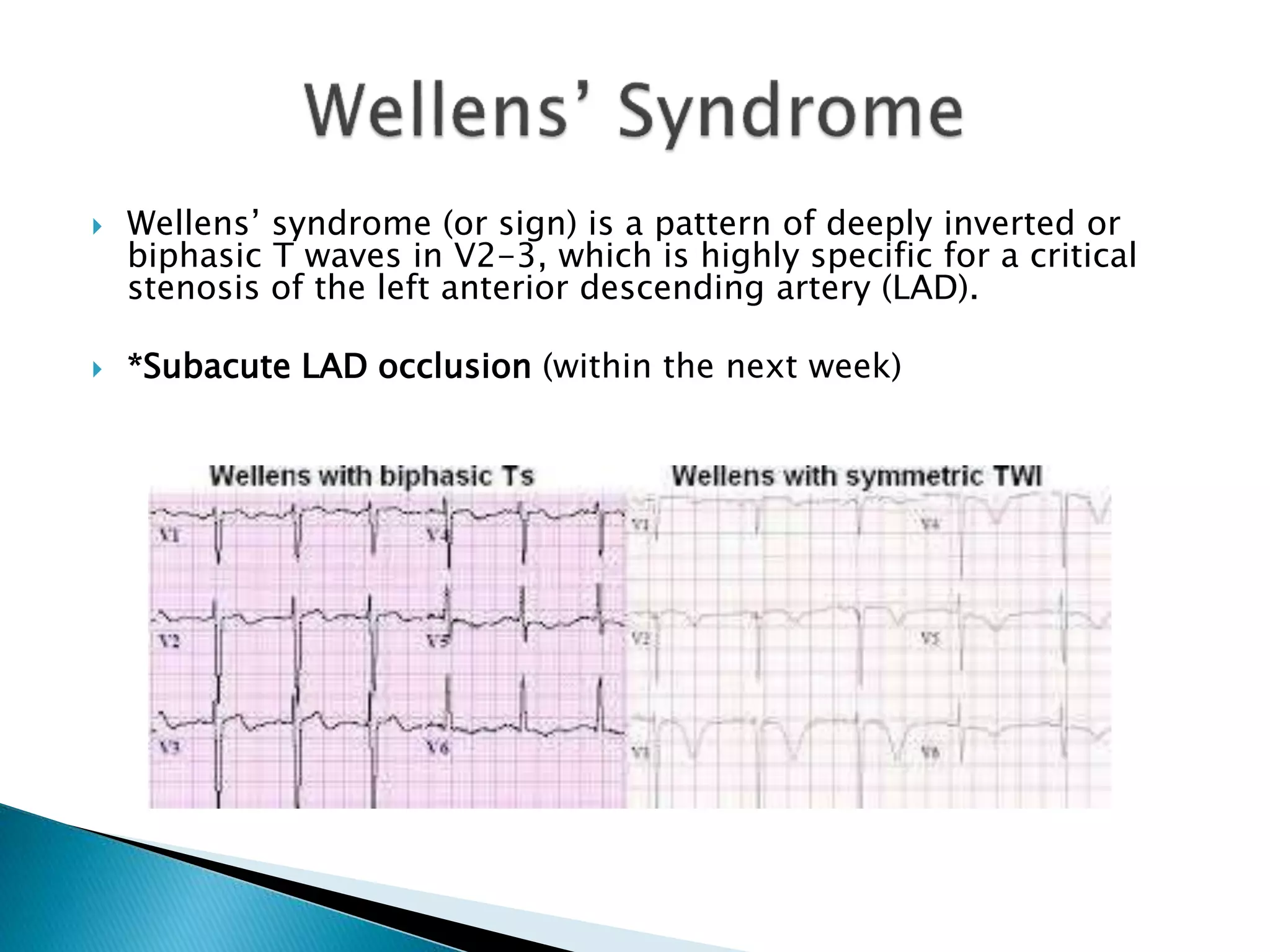


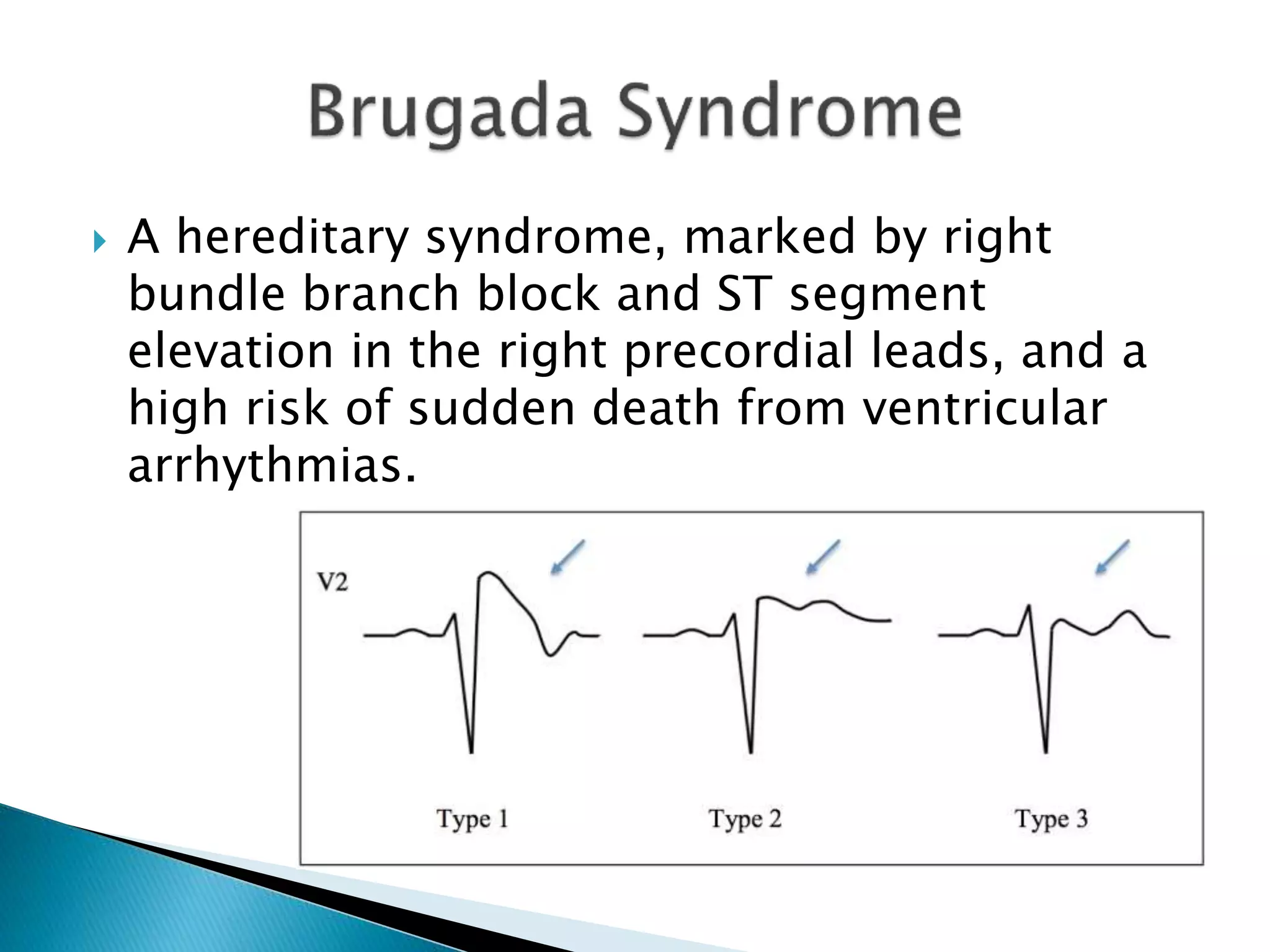











The document discusses various ECG findings that indicate ST-Elevation Myocardial Infarction (STEMI), including criteria for diagnosing STEMI with ST segment elevation and reciprocal changes in contiguous leads. It outlines specific ECG features for different types of myocardial infarction, the importance of certain wave characteristics, and guidelines for differentiating between STEMI and pericarditis. Additionally, it highlights specific syndromes related to coronary artery issues and provides diagnostic criteria for acute conditions.



































































