Downloaded 297 times
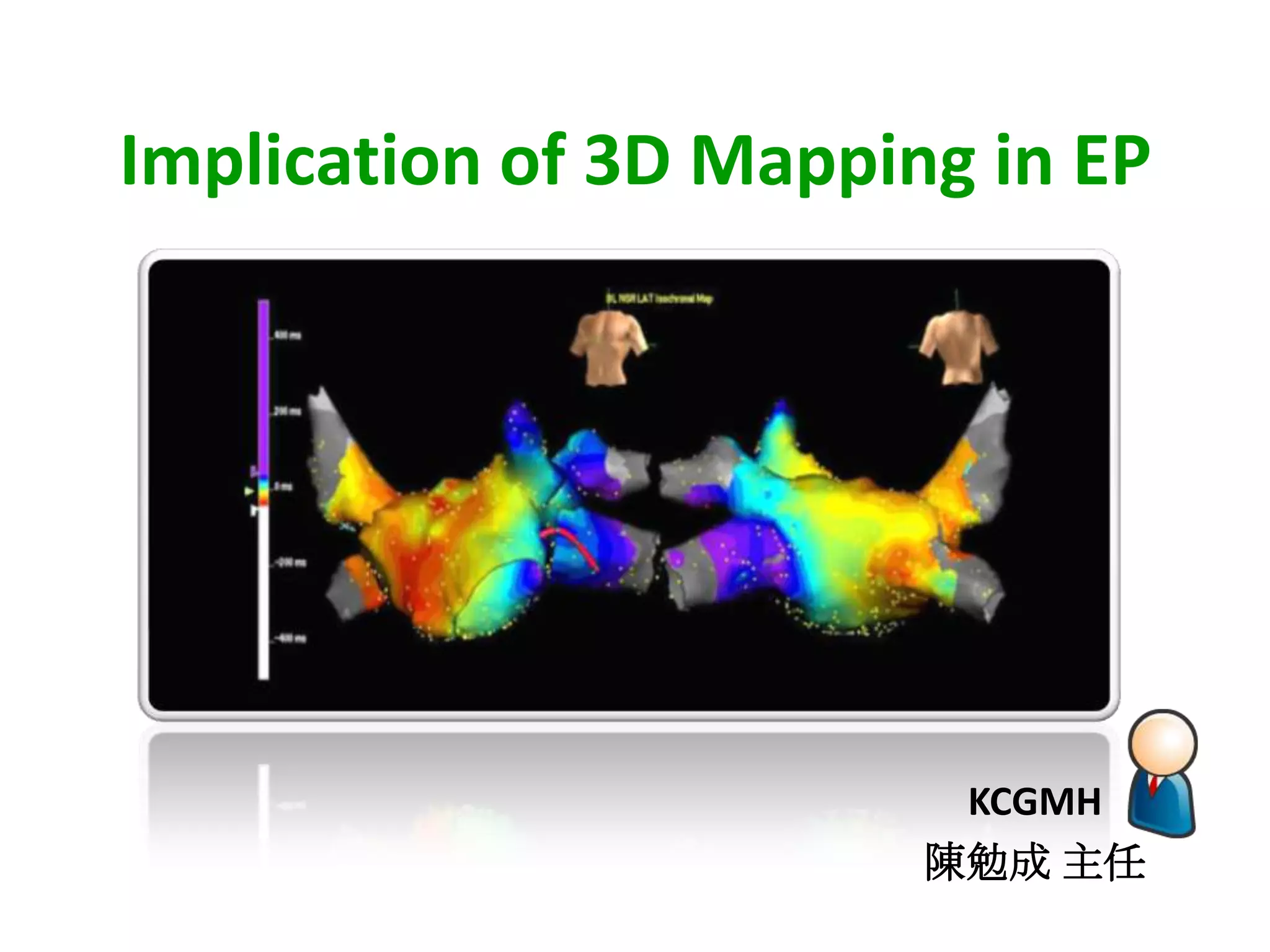
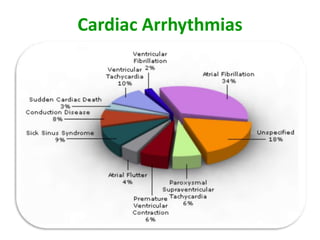
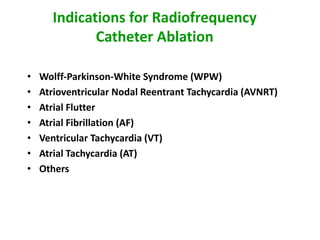
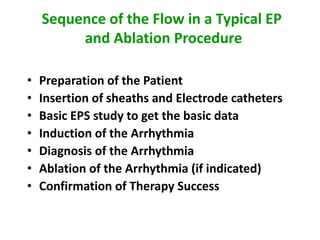
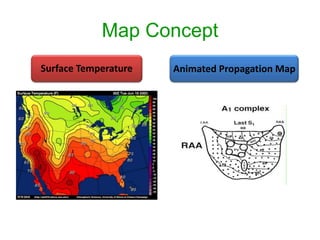
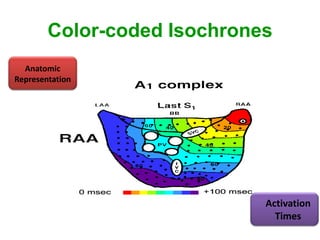
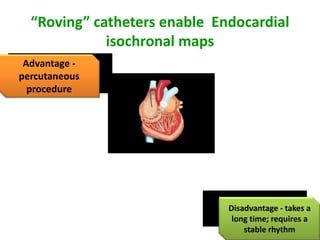
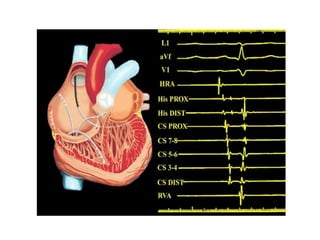
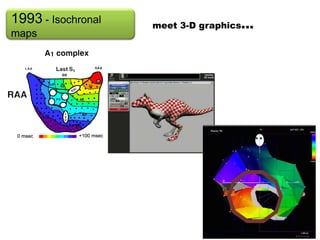



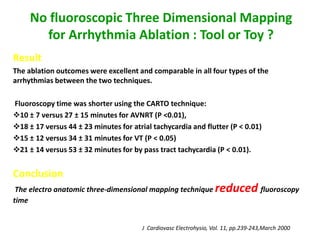


This document discusses the implications of 3D mapping in electrophysiology procedures. It provides an overview of common arrhythmias treated with catheter ablation such as WPW syndrome, AVNRT, atrial flutter, and atrial fibrillation. It describes the typical sequence of an EP study and ablation procedure. It also discusses classification of tachycardias as focal or macroreentrant, and different reentry patterns. The document highlights the development of 3D mapping technologies including contact and non-contact mapping systems, and their ability to create 3D geometry and electroanatomic maps with integration of CT/MRI images. It reviews studies validating the reduction of fluoroscopy time with 3D mapping approaches.