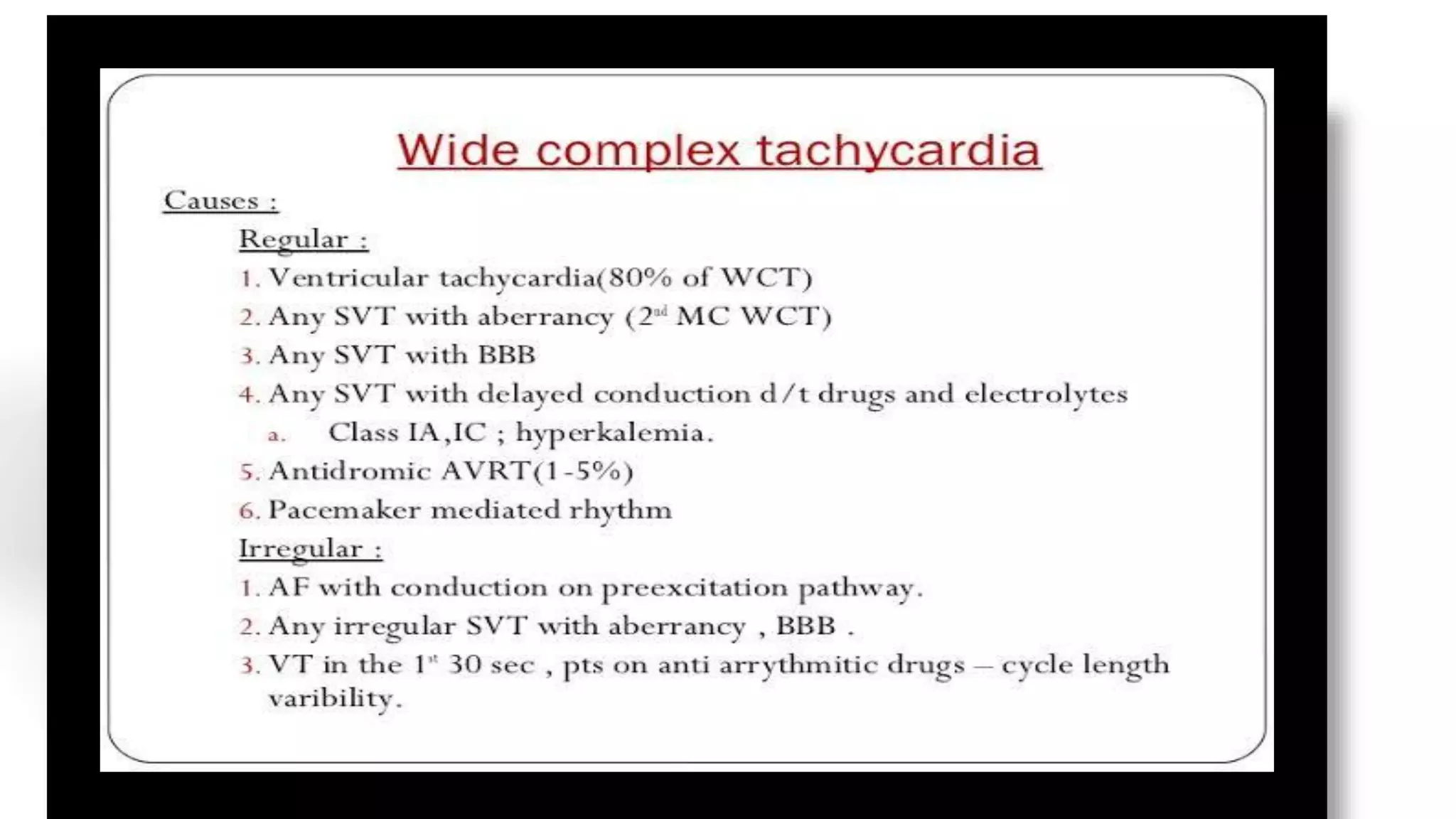
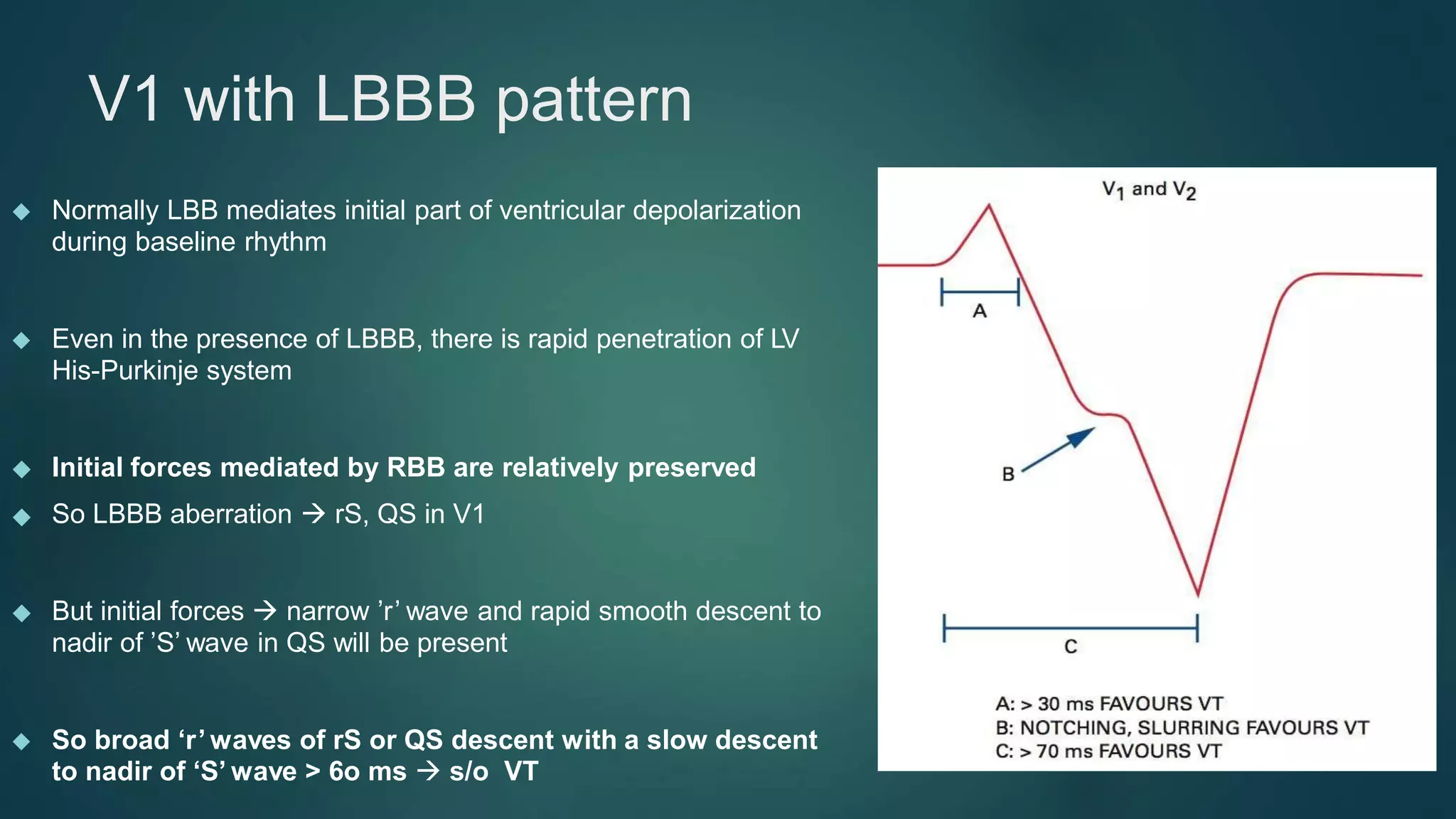
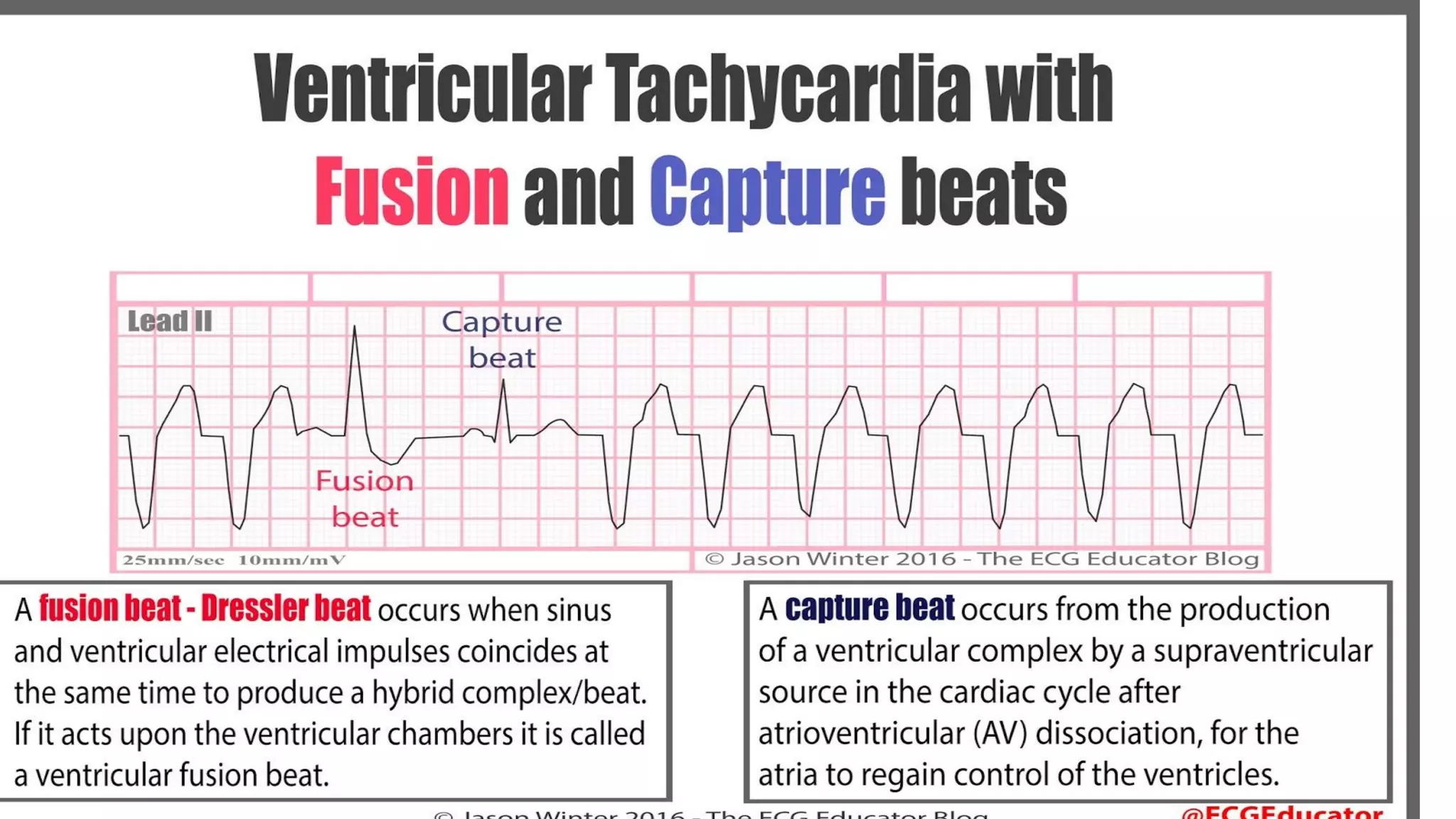
This document provides an overview of the approach to evaluating and diagnosing wide complex tachycardias. It begins with definitions of terms like wide complex tachycardia, ventricular tachycardia, and supraventricular tachycardia. It then discusses the importance of making an accurate diagnosis to avoid inappropriate treatment. Various ECG criteria are presented to help distinguish ventricular from supraventricular rhythms based on features like AV dissociation, QRS morphology, axis, and precordial patterns. Specific criteria for right bundle branch block and left bundle branch block morphologies are also outlined. The document emphasizes taking a stepwise approach and considering clinical history in narrowing the differential diagnosis of wide complex tachycardias.