Downloaded 371 times
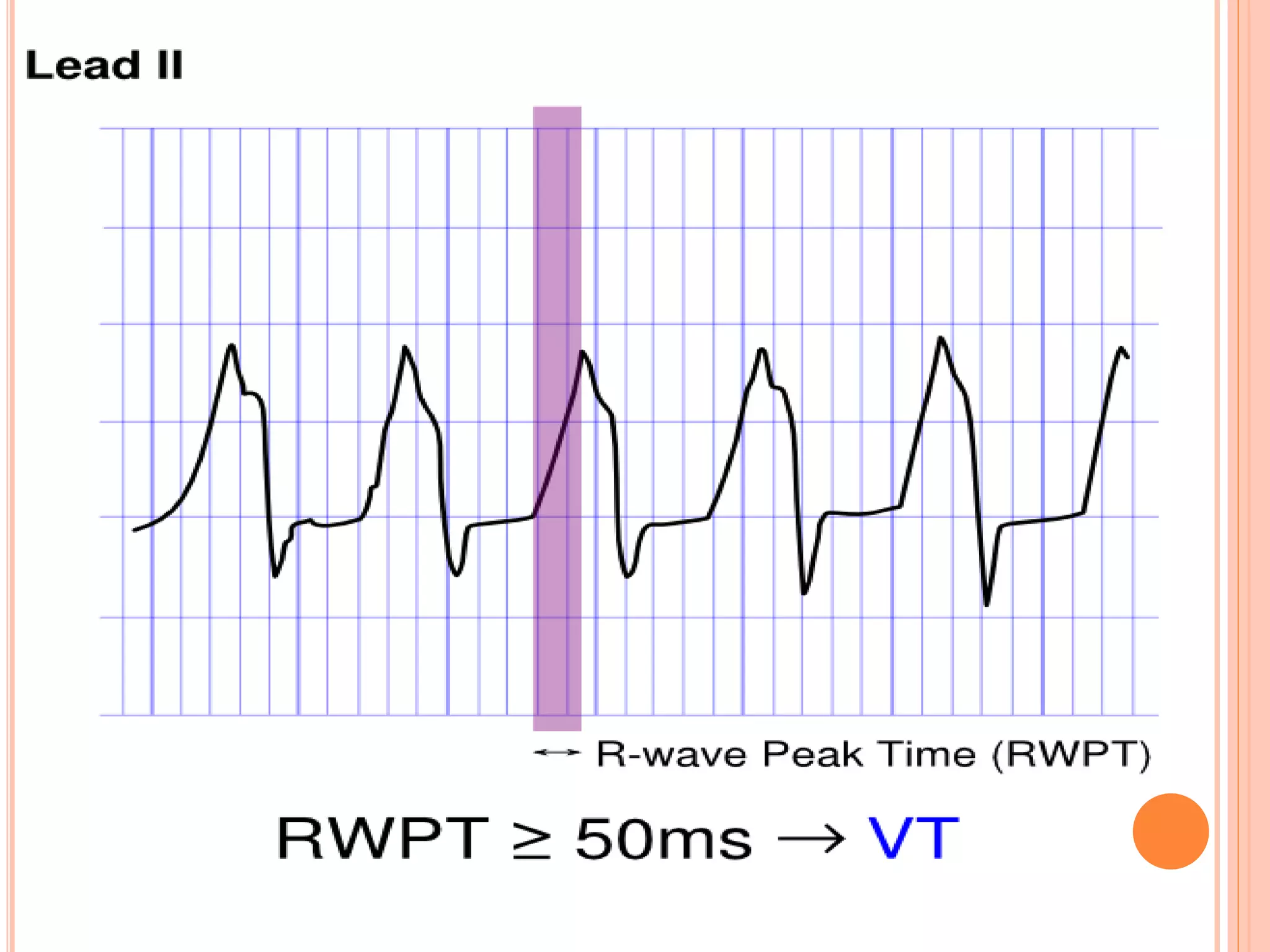
![ULTRASIMPLE BRUGADA CRITERION: RW TO PEAK
TIME (RWPT)
In 2010 Joseph Brugada et al. published a new
criterion to differentiate VT from SVT in wide
complex tachycardias: the R wave peak time in
Lead II [4].
They suggest measuring the duration of onset of
the QRS to the first change in polarity (either nadir
Q or peak R) in lead II. If the RWPT is ≥ 50ms the
likelihood of a VT very high (positive likelihood ratio
34.8).](https://image.slidesharecdn.com/vtinstructurallynormalheart-150819183228-lva1-app6891/75/VT-in-structurally-normal-heart-15-2048.jpg)


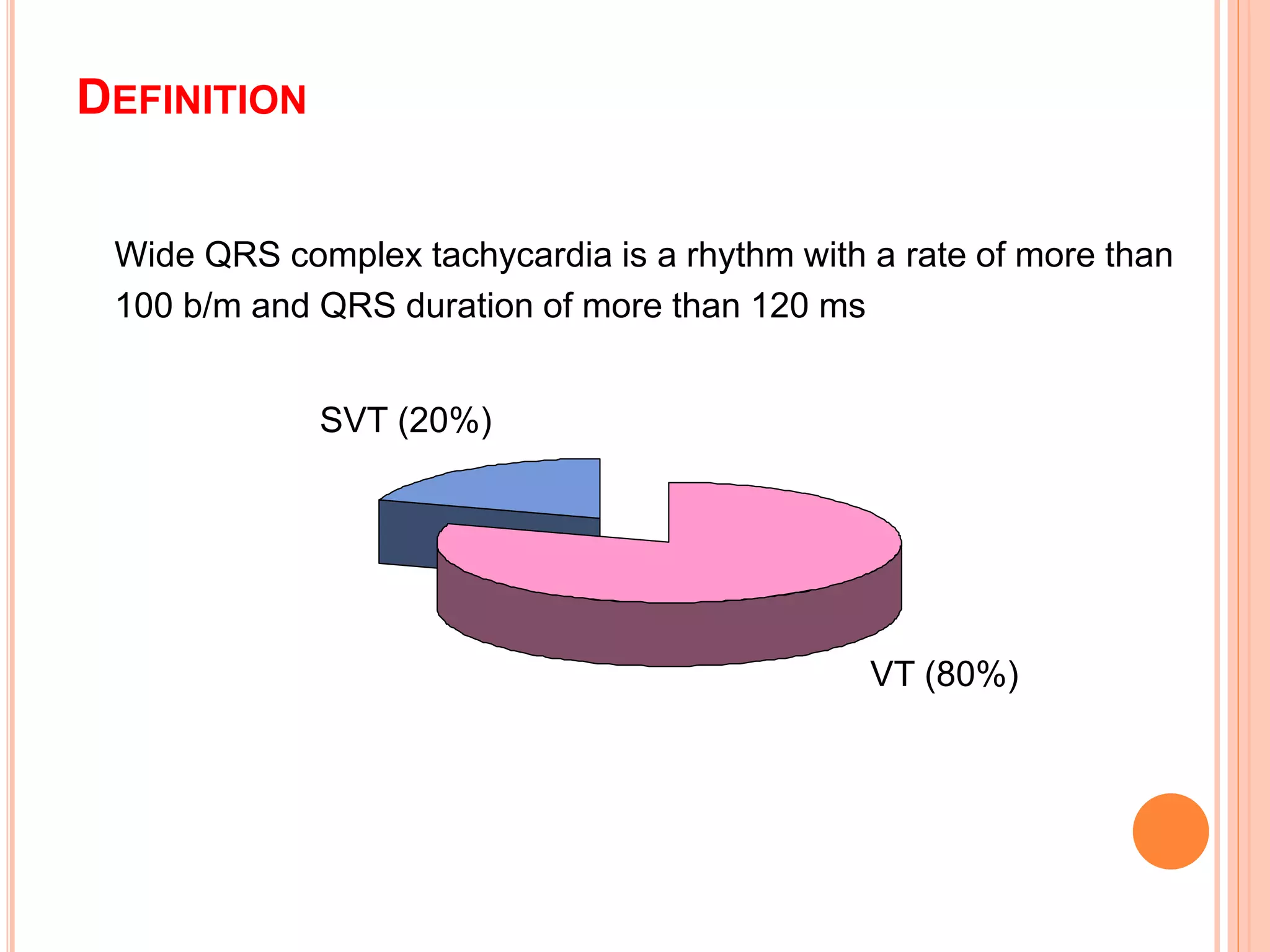
The document discusses ventricular tachycardia (VT) in patients with structurally normal hearts, outlining its definitions, types, diagnosis, and management strategies. It emphasizes the differentiation between VT and supraventricular tachycardia (SVT), as well as the clinical significance of ECG patterns and recent algorithms for improved diagnosis. Treatment options range from acute interventions like carotid sinus massage to long-term strategies including beta-blockers, catheter ablation, and consideration for implantable cardioverter-defibrillators in high-risk cases.