Downloaded 68 times





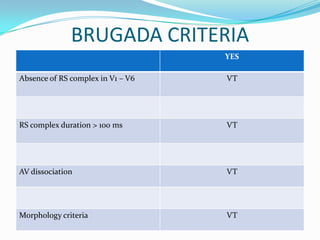

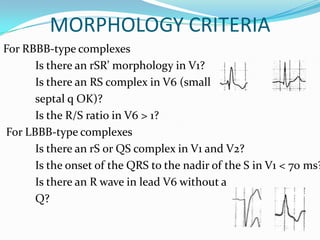
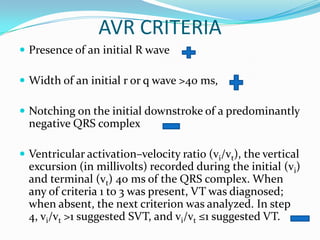








A 22-year-old male presented with acute onset breathlessness, palpitations, profuse sweating, and vague chest discomfort for 1 hour. His ECG showed tachycardia at 200 bpm with a regular rhythm, right bundle branch block pattern, and extreme northwest axis. This case report discusses the differential diagnosis and criteria used to differentiate ventricular tachycardia from supraventricular tachycardia with aberrancy based on the ECG findings. Key criteria evaluated include Brugada criteria, AVR criteria, morphology, axis, and presence of fusion or capture beats. The conclusion is that while no single criteria is definitive, if there is any doubt the rhythm should be treated as ventricular tachycard




























































