Primary Survey
A :Can speak , No tenderness at posterior midline
B : Normal chest movement , Equally breath sounds
both lung , CCT - negative
C : BP 117/77 mmHg , PR 74 bpm , no active bleeding
D : E4V5M6 , pupil 3 mm RTLBE
E : no external wound , tenderness and limit ROM due
to pain at Rt wrist
4.
Secondary survey –
History
0Allergy : no drug or food allergy
0 Medication: no current medication
0 Past illness: No underlying diseases
0 Last meal : 12.00 , 23 November 2017
0 Event : 1 ชั่วโมงก่อนมาโรงพยาบาล ขณะเรียนลูกเสือ ผู้ป่วยหกล้ม ข้อมือขวา
กระแทกพื้น หลังจากล้ม ปวดและบวมที่ข้อมือขวา ขยับได้น้อยลง ไม่ผิดรูป ไม่ชา
ไม่อ่อนแรง ไม่มีไข้
5.
Secondary survey -
Examination
0Head & Maxillofacial :
no wound , no ecchymosis
0 C-spine & Neck :
No wound at neck , can movement without pain
0 Chest :
Equally breath sounds both lung
0 Abdomen & Pelvis :
soft , not tender
0 Perineum/Rectum :
can’t evaluate
6.
Secondary survey -
Examination
0Musculoskeletal:
Rt forearm – No deformities , mild swelling ,
marked tenderness at radial aspect of wrist ,
limit ROM due to pain , able to flex and extend all digits ,
unable to supinate and pronate
Neurovarscular – Radial and Ulnar pulse 2+
Motor - Can’t flex wrist , able to flex all digits
Sensory - Intact , no numbness
0Neurologic :
GCS : E4V5M6
Management
0 Pain control
0Pethidine 25 mg iv stat
0 Closed reduction with short arm AP slab
and arm sling
0 Advice about slab care and complication
0 Follow up 1 wk. (28.11.2017) with filming
0 HM
0 Paracetamol (325) 1 tab oral prn for pain
q 4-6 hrs
13.
0 Plain filmRt Wrist
AP , lateral view
after reduction and
slab insertion
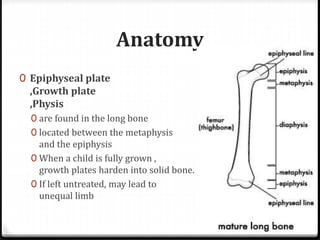
Anatomy
0 Epiphyseal plate
,Growthplate
,Physis
0 are found in the long bone
0 located between the metaphysis
and the epiphysis
0 When a child is fully grown ,
growth plates harden into solid bone.
0 If left untreated, may lead to
unequal limb
Epidermiology
0 15 –30 % of fracture in children
0 The incidence of growth plate fractures peaks in
adolescence.
0 Usually happen with sport training/activity/
MC accident (วัยรุ่น) or Fall from height (เด็กเล็ก)
18.
Clinical Manifestation
0 Agrowth plate fracture usually causes Persistent or
severe pain.
0 Other common symptoms include :
0 Visible Deformity
0 An ability to move or put pressure on the limb
0 Swelling , Warmth , and Tenderness in the area around
the end of the bone, near the bone
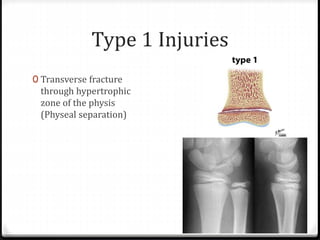
Type 1 Injuries
0Transverse fracture
through hypertrophic
zone of the physis
(Physeal separation)
22.
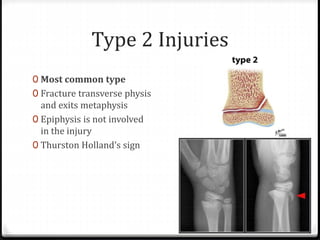
Type 2 Injuries
0Most common type
0 Fracture transverse physis
and exits metaphysis
0 Epiphysis is not involved
in the injury
0 Thurston Holland’s sign
23.
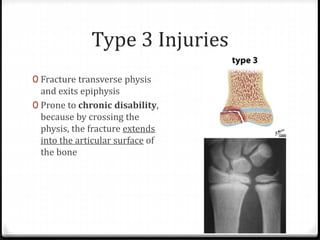
Type 3 Injuries
0Fracture transverse physis
and exits epiphysis
0 Prone to chronic disability,
because by crossing the
physis, the fracture extends
into the articular surface of
the bone
24.
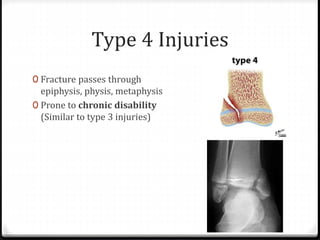
Type 4 Injuries
0Fracture passes through
epiphysis, physis, metaphysis
0 Prone to chronic disability
(Similar to type 3 injuries)
25.
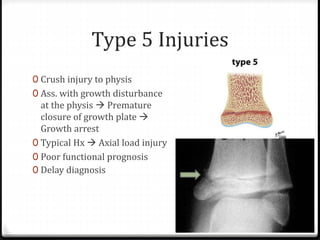
Type 5 Injuries
0Crush injury to physis
0 Ass. with growth disturbance
at the physis Premature
closure of growth plate
Growth arrest
0 Typical Hx Axial load injury
0 Poor functional prognosis
0 Delay diagnosis
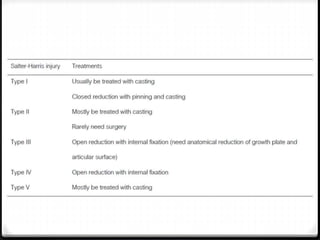
Non operative
0 Salter-Harristype 1 & 2 can be treat with
conservative treatment
0 Reduction and immobilization with Splint/Slab
0 Follow up every week and Splint up to
3-4 weeks
30.
0 Epiphyseal plateinjury at Rt. distal end radius
( Salter-Harris II )
0 Closed reduction & Short arm cast no distal ulnar fx
0 Closed reduction & Long arm cast distal ulnar fx
0 3-4 wks


























![Extern conference. tung[1]](https://cdn.slidesharecdn.com/ss_thumbnails/externconference-161129124720-thumbnail.jpg?width=640&height=640&fit=bounds)












































