Patient Profile
• A13 Thai boy
• Cause of injury : MC ชนกระกระบะ
• Time : 11.30 27 September 2017
3.
Primary survey atMNRH
A On Hard collar, On ETT
B Trachea in midline, symmetrical
movement, equal breath sound breath
sound both lung, CCT negative
C BP 120/80 mmHg, P 80 bpm
D E2VTM6, pupil 3 mm RTLBE
Secondary survey atMNRH
• Allergy no drug allergy
• Medication no current medication
• Past History no underlying disease
• Last meal 9.00
• Event ผู้ป่วยขับรถ MC ชนกับรถกระบะ สลบ ไม่ทราบระยะเวลา
มีบาดแผลตามร่างกาย เหงื่ออก ตัวเย็น ปัสสาวะ อุจจาระราด
EMS ออกรับที่ รพช. On hard collar ใส่ ETT แล้ว
refer มา
6.
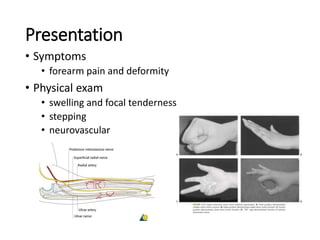
Physical Examination
• Vitalsign T 37oC BP 120/80 Pulse 80 bpm RR on ETT
• Head & Maxillofacial
No external wound, no contusion,
no tenderness, no facial deformity
• Cervical spine & Neck
On hard collar
7.
Physical Examination
• Chestno contusion, trachea in midline,
symmetrical movement, clear &
equal breath sound both lung,
Normal S1 S2 no murmur
• Abdomen Contusion at anterior abdomen
No distended, hypoactive BS,
soft, no guarding
8.
Physical Examination
• PerineumNo seen external wound
• MSK Laceration wound 5 cm, avulsion
wound 5 cm with exposed tendon
on right leg, DPA & PTA 2+, sensory
cannot evaluate
• Neurologic E3VTM5, pupil 3mm RTLBE,
power at least gr 3 all extremities,
sensory cannot evaluate, PR good
sphincter tone
9.
Problem List
• R/OC-spine injury
• Mild Head Injury (moderate risk)
• Blunt abdominal injury
• Tear Achilles tendon Rt
10.
Management
• Admit ICUtrauma
• Consult neuro sx ; CT brain Observe neurosign
• Consult trauma ; set OR for explor laparotomy
• Consult ortho ; Set OR for repair tendon
11.
Post operation
• Notify
หลังจากผ่าตัด1 สัปดาห์ ผู้ป่วยปวดข้อมือทั้ง 2 ข้าง หลังจากถูก physical restrain
ขยับข้อมือได้ ไม่ชา กดเจ็บตรงบริเวณข้อมือ
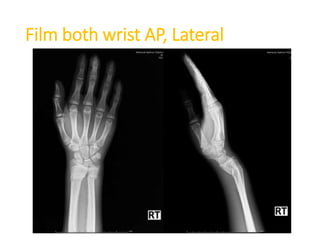
PE both wrist
tenderness, no swelling, no warm, dorsal deformity,
with stepping, Limit ROM on active motion full ROM by
passive, sensory intact, ulnar & radial pulse 2+
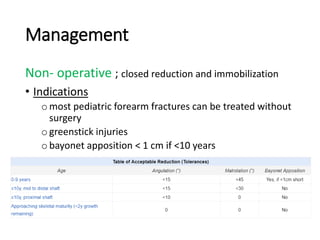
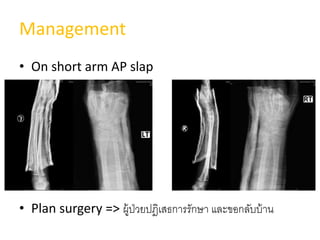
Management
Non- operative ;closed reduction and immobilization
• Indications
omost pediatric forearm fractures can be treated without
surgery
ogreenstick injuries
obayonet apposition < 1 cm if <10 years
20.
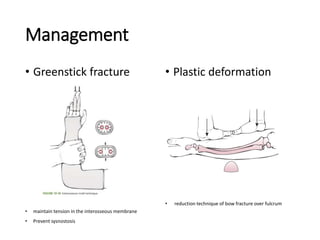
Management
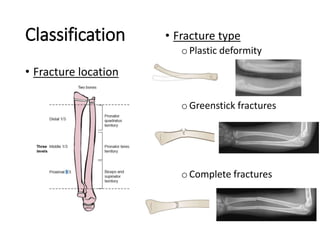
• Greenstick fracture
•maintain tension in the interosseous membrane
• Prevent sysnostosis
• Plastic deformation
• reduction technique of bow fracture over fulcrum
21.
Management
• Casting
• longarm cast/slap 4-6 wks, possible conversion to short
arm cast after 4wk
(depending on fracture type and healing response)
• F/U in 1st wk ; ดูเฝือก
• F/U every 2 wk ; พิจารณาถอดเฝือกเมื่อกระดูกเชื่อมติดกันดี
22.
Management
Operation
Indication
• unacceptable alignmentfollowing closed reduction
oangulation >15°, rotation >45° in children <10y
oangulation >10°, rotation >30° in children >10y
obayonet apposition in children older than 10 years
• both bone forearm fractures in children> 13