Primary survey
• A: Can talk, no midline tenderness along c-spine
• B : Negative chest compression test, trachea in
midline, equal chest movement and equal breath
sound both lungs
• C : BP 125/74 PR 102 /min
• D : E4V5M6, pupils 3 mm RTLBE
• E : Right forearm swelling, no wound, sensory
intact, capillary refill< 2 sec, passive stretch test
negative
6.
Secondary survey
A :no food and drug allergy
M : no current medication
P: no underlying disease
L : last meal 3 hr. PTA
E : ขณะวิ่งเล่นกับเพื่อน หกล้ม แขนขวากระแทกพื้น มีอาการปวดบวม
แขนขวา ไม่มีบาดเจ็บที่อื่น
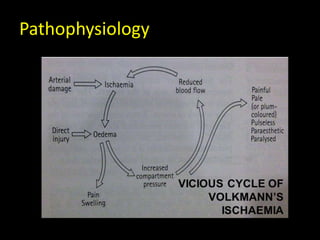
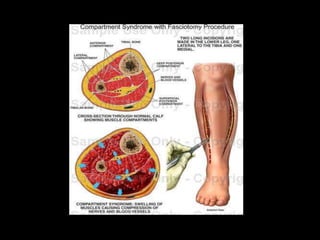
Definition
- Elevated tissuepressure within a closed fascial
space
- Ruduces tissue perfusion – ischemia
- Results in cell death – necrosis
True Orthopaedic Emergency
Signs and symptoms
5P’s
1. Pain : The earliest sign
2. Paraesthesia
3. Pallor
4. Paralysis
5. Pulselessness
Signs :
1. tight swelling
2. Loss of strength
3. Loss of sensation
4. Blister
(presence of a pulse does not exclude the diagnosis)
23.
The earliest sign: PAIN
• Pain that out of proportion to the injury
• Describe as ‘bursting’ sensation
• Pain that is not responsive to the normal
dosage of pain medication
• Severe pain with passive stretch
24.
Diagnosis
• Passive stretchingof fingers or toes (muscle
stretch)will lead to severe pain (diagnostic
sign)
• Compartment syndrome is a clinical diagnosis
• Never wait for signs of ischemia (5 Ps) :
irreversible damage
26.
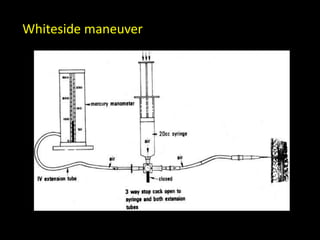
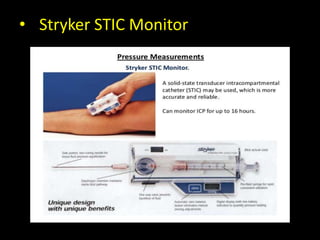
For obtunded, intubated,or unreliable patients
who have a swollen extremity but who
otherwise cannot be evaluated
Complications
• Acute renalfailure secondary to
rhabdomyolysis
• Disseminated intravascular coagulation
• Volkmann’s contracture (where infarcted
muscle is replaced by inelastic fibrous tissue)
• Amputation
37.
• Compartment syndromeis a serious
syndrome, Which needs to be diagnosed
early.
• Palpable pulse doesn’t exclude compartment
syndrome
• If diagnosis and fasciotomy were done within
24 hrs, the prognosis is good.
• If delayed, complications will develop.
The earlier you diagnose, the safer you are
If not sure Admit patient for Close monitoring
Take home message!!
































![Angiodysplasia[1]](https://cdn.slidesharecdn.com/ss_thumbnails/angiodysplasia1-190610163612-thumbnail.jpg?width=640&height=640&fit=bounds)
























