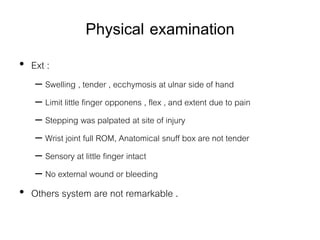
Physical examination
• Ext:
– Swelling , tender , ecchymosis at ulnar side of hand
– Limit little finger opponens , flex , and extent due to pain
– Stepping was palpated at site of injury
– Wrist joint full ROM, Anatomical snuff box are not tender
– Sensory at little finger intact
– No external wound or bleeding
• Others system are not remarkable .
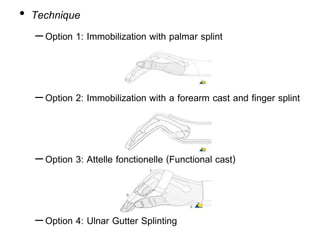
• Technique
–Option 1:Immobilization with palmar splint
–Option 2: Immobilization with a forearm cast and finger splint
–Option 3: Attelle fonctionelle (Functional cast)
–Option 4: Ulnar Gutter Splinting
16.
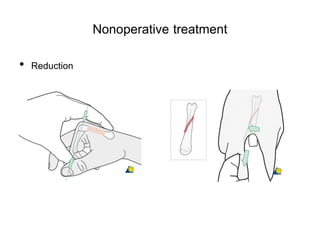
Operative treatment
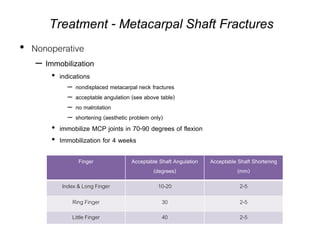
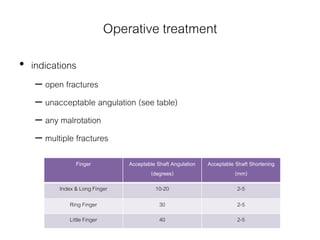
• indications
–open fractures
– unacceptable angulation (see table)
– any malrotation
– multiple fractures
Finger Acceptable Shaft Angulation
(degrees)
Acceptable Shaft Shortening
(mm)
Index & Long Finger 10-20 2-5
Ring Finger 30 2-5
Little Finger 40 2-5
17.
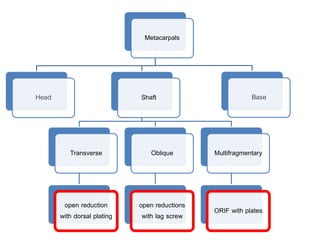
Techniques of Operation
•closed reduction percutaneous pinning
• open reductions with lag screw
– can use multiple lag screws for long spiral fractures
• try to get at least two lag screws
• open reduction with dorsal plating
– works best for transverse fractures
– try to cover plate with periosteum to prevent tendon irritation
– begin early motion to prevent tendon irritations