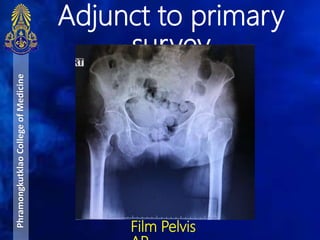
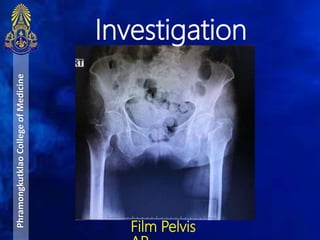
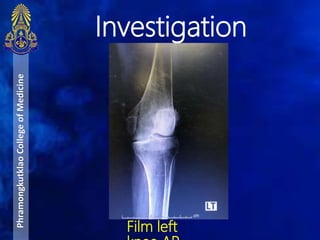
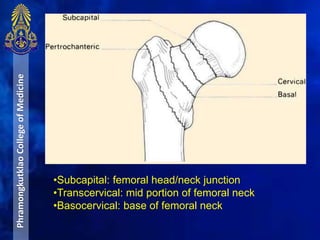
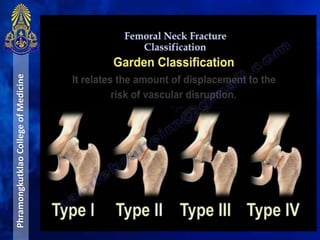
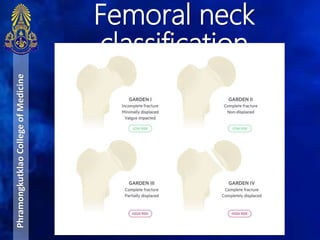
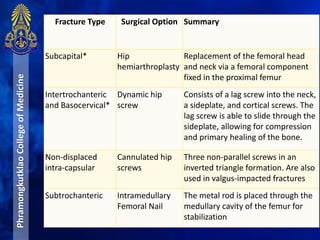
An 81-year-old Thai woman presented to the hospital with left hip pain after falling three days prior. Imaging revealed a Garden type 3 fracture of the left femoral neck. She was diagnosed with a displaced left femoral neck fracture. Her treatment plan included pain control, skin traction of the left leg, and a left bipolar hemiarthroplasty surgery. Femoral neck fractures typically result from low-energy falls in older patients and require prompt surgical management to reduce complications.























































![INJURIES AROUND HIP [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/injuriesaroundhipautosaved-240206110505-4ae81da1-thumbnail.jpg?width=640&height=640&fit=bounds)







































