SECONDARY SURVEY
• A: No allergy
• M: No current medication
• P : unknown U/D and Last TT vaccine > 5 ปี
• L : last meal 12.00 น. (เหล้า+กับแก้ม)
• E : 2 hr PTA ดื่มสุราจนเมาแล้วขับ MC (ไม่สวมหมวกนิรภัย)ชนรถหกล้อ
กระเด็นหัวเข่าขวากระแทกพื้น สลบ จาเหตุการณ์ไม่ได้ มีบาดแผลฉีดขาดที่หัวเข่ามี
เลือดไหลไม่หยุด ขยับเข่าขวาไม่ได้เนื่องจากปวด เดินลงน้าหนักไม่ได้ ไม่มีอ่อนแรง ไม่มี
ชาปลายเท้า จากนั้นถูกส่งตัวมาโรงพยาบาล
9.
PHYSICAL EXAMINATION
• GA: A Thai man good consciousness , well cooperative
• V/S : BT 37.4 C PR 88 bpm RR 20 bpm BP 146/84
mmHg
• HEENT : not pale conjunctivae , anicteric sclerae , LN
can’t palpable
• Heart : normal S1S2 no murmur
• Lung : clear both lungs
10.
PHYSICAL EXAMINATION
•Extremities :
-LW 8*6 cm with dirty wound deep to bone
- Limit ROM at Rt.knee joint
- Tender around Rt.knee
- Unable to perform straight leg raising
Pulse :
Neuro : grossly intact
Right Left
dorsalis pedis artery (DPA) 2+ 2+
posterior tibial artery (PTA) 2+ 2+
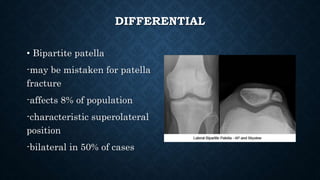
DIFFERENTIAL
• Bipartite patella
-maybe mistaken for patella
fracture
-affects 8% of population
-characteristic superolateral
position
-bilateral in 50% of cases
TREATMENT (NONOPERATIVE)
• Nonoperative: knee immobilized in extension
(cylinder cast) and full weight bearing
Indications :
-intact extensor mechanism (patient able to
perform straight leg raise)
-nondisplaced or minimally displaced fractures
-vertical fracture patterns
18.
TREATMENT (OPERATIVE)
• Indicationfor surgery
-extensor mechanism failure (unable to perform straight leg
raise)
-open fractures
-fracture articular displacement >2mm
-displaced patella fracture >3mm
-patella sleeve fractures in children
19.
MANAGEMENT
• Admit
• NPO
•5%DN/2 1000 ml IV rate 80 ml/hr
• dT booster 0.5ml IM
• Set OR for DB with arthrotomy with K-wire
• Cefazolin 1g IV q 6 hr
• Gentamicin 240 mg IV q OD