Primary survey
A :able to talk, airway patent, not tender along c-spine
B : no tachypnea, trachea in midline, equal chest expansion, equal
breath sound
C : BP 116/61 mmHg, PR 72/min, cap. refill < 2 sec, no external
wound, no active bleeding
D : E4,V5,M6, pupil 2 mm RTLBEs
E : tender Lt. wrist, mild swelling, limit ROM due to pain, NV intact
4.
Secondary survey
A :no allergy
M : no current medication
P : no U/D
L : 20.00
E : เสียหลักตกจากรถไส หงายหลัง ใช้ข้อมือซ้ายยันพื้น (17.00 น.) ไม่มีศรีษะกระแทกพื้น
ไม่สลบ จาเหตุการณ์ได้ ปวดข้อมือซ้าย ขยับไม่ได้ ไม่ชา
5.
Physical examination
V/S :BT 36.1 C, BP 116/16 mmHg, PR 72/min, RR 16/min
GA : A young Thai man, good consciousness
HEENT : not pale conjunctivae, anicteric sclerae
Neck : not tender at posterior midline
Heart : normal S1S2, no murmur
Lungs : equal breath sound, clear
6.
Physical examination
Abdomen :no distion normoactive bowel sound,
soft, not tender
Back : not tender along spine
Extremities : tender at Lt. radial styloid, mild
swelling, limit ROM due to pain, NV intact
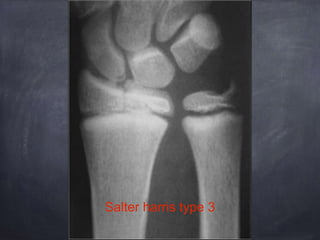
Distal radius fracture
Epidemiology
Incidence
common- forearm fractures in total account for approximately
40% of all pediatric long bone fractures
distal radius (and ulna) is the most common site of pediatric
forearm fractures.
male > female (male 2-3 times more common than female)
14.
Distal radius fracture
Demographics
mostcommon during metaphyseal growth spurt
peak incidence occurring from:
10-12 years of age in girls
12-14 years of age in boys
most common fracture in children under 16 years old
15.
Distal radius fracture
Pathophysiology
mechanism
usuallyfall on an outstretched hand, extended at wrist
often during sports or play
remodeling
greatest closer to physis and in plane of joint (wrist) motion
sagittal plane (flexion/extension)
least for rotational deformity
16.
Distal radius fracture
Anatomy
Distalradius physis
contributes 75% growth of the radius
contributes 40% of entire upper extremity
growth at a rate of ~ 5.25mm per year
Metaphyseal fracture most common, followed by physeal