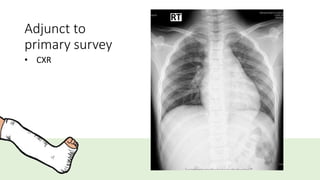
Primary survey atMNRH
• A – can talk, no posterior midline neck tenderness, full ROM of neck
• B – trachea in midline, spontaneous breathing, CCT negative, clear
and equal breath sound
• C – BP 110/72 mmHg, PR 108 bpm, no external bleeding, PCT
negative
• D – E4V5M6 pupils 2mm RTLBE
• E – left elbow deformity with swelling and tender with limit ROM
Secondary survey
• A– no drug and food allergy
• M – no current medication
• P – no underlying disease, no history of surgery
• L – 18.00 8/3/61
• E – ตกจากกองดิน สูง1.5เมตร ศอกข้างซ้ายผิดรูป บวม ปวด ขยับไม่ได้ ไม่มีบาดแผลภายนอก
8.
Head-to-toe examination
• Headand maxillofacial
• No wound, no facial deformity, no ecchymosis
• C-spine and neck
• No wound, no C-spine tenderness, full active ROM of neck
• Chest
• Trachea in midline, clear and equal breath sound both lungs,
CCT negative
• Abdomen and pelvis
• Not distend, no wound, soft, not tender, normoactive bowel,
PCT negative
9.
Head-to-toe examination
• Musculoskeletal
•Deformity, tender and swelling at left elbow, limit ROM of left elbow
• Radial pulse 2+, capillary refill <2 sec, normal pinprick sensation
• Neurologic
• E4V5M6, pupils 2 mm RTLBE
• Motor grade V all except left elbow due to pain and deformity
• Perineum and rectum
• No ecchymosis
Epidemiology
• Children 5- 7 years old
• Male = Female
• Types
• Extension - most common (95-98%)
• Flexion type (<5%)
• Mechanism of injury – fall on outstretched hand
19.
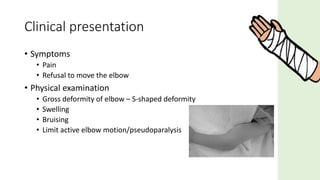
• Symptoms
• Pain
•Refusal to move the elbow
• Physical examination
• Gross deformity of elbow – S-shaped deformity
• Swelling
• Bruising
• Limit active elbow motion/pseudoparalysis
Clinical presentation
20.
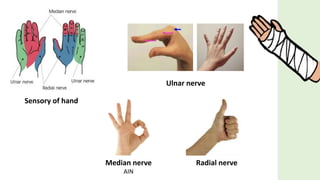
• Neurapraxia –almost all resolve spontaneously
• Anterior interosseous nerve neurapraxia (branch of median n.)
• most common
• Radial nerve palsy
• Ulnar nerve palsy
• Flexion type
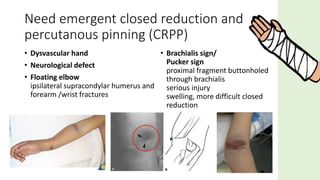
• Vascular injury (1%) – rich in collateral circulation
Associated injuries
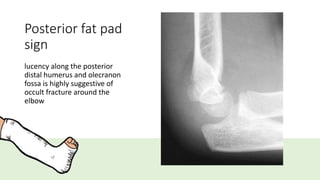
Posterior fat pad
sign
lucencyalong the posterior
distal humerus and olecranon
fossa is highly suggestive of
occult fracture around the
elbow
24.
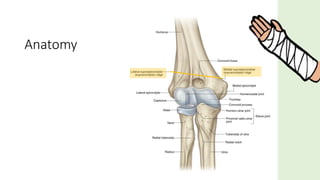
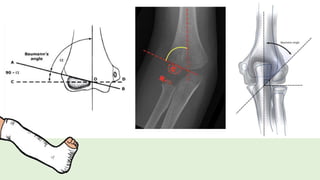
Baumann’s angle
• Humeral-capitellarangle
• Humeral axis and a straight line through the epiphyseal plate of the
capitellum
• Normal: 64 - 81° or differ 5° between the two sides
26.
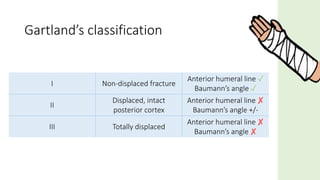
Gartland’s classification
I Non-displacedfracture
Anterior humeral line ✓
Baumann’s angle ✓
II
Displaced, intact
posterior cortex
Anterior humeral line ✘
Baumann’s angle +/-
III Totally displaced
Anterior humeral line ✘
Baumann’s angle ✘