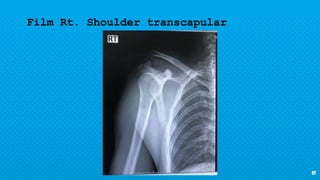
- The patient is a 38-year-old Thai man who was in a motorcycle accident while intoxicated. He hit a footpath and was thrown from the motorcycle, landing on his right shoulder on the road without a helmet.
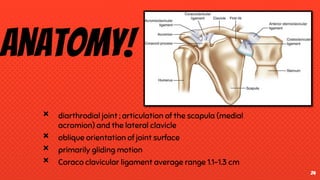
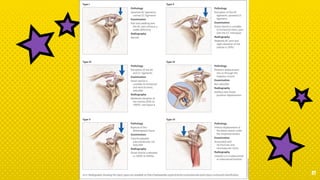
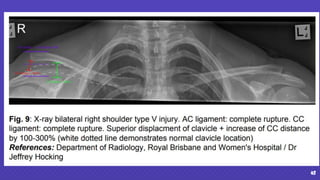
- On examination, he had pain and limited movement in his right shoulder. Imaging showed a grade V injury of the right acromioclavicular joint with disruption of the acromioclavicular and coracoclavicular ligaments.
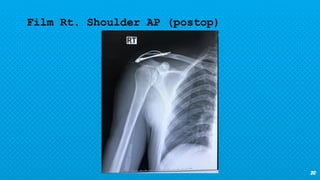
- He underwent open reduction and internal fixation surgery with tightrope fixation of the right acromioclavicular joint.