Downloaded 1,260 times

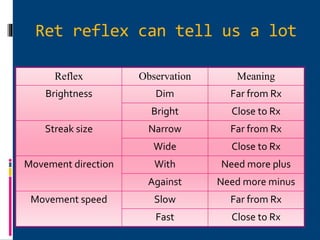
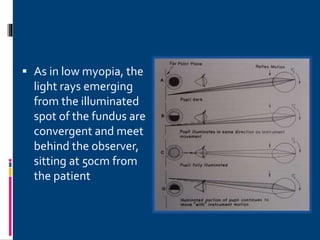
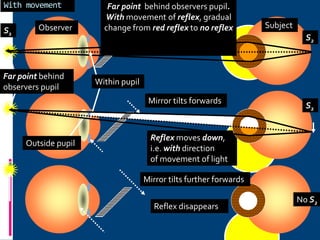
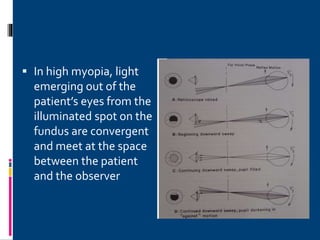
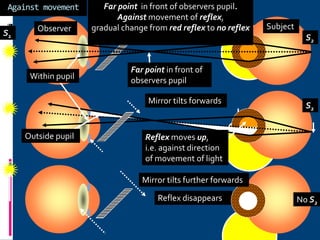

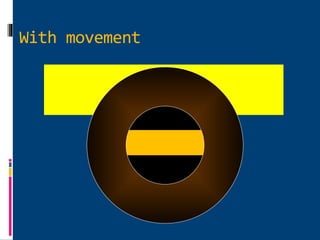
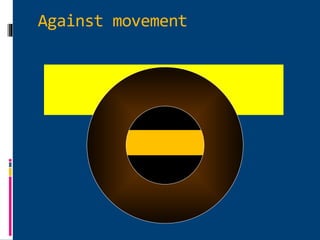
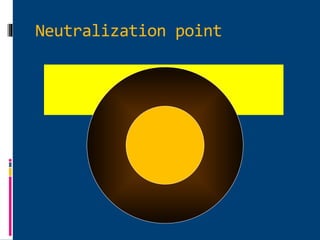
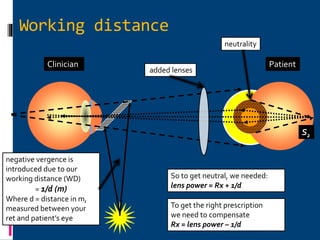
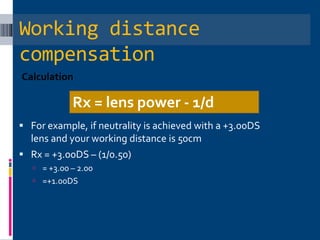
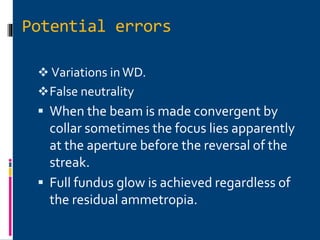
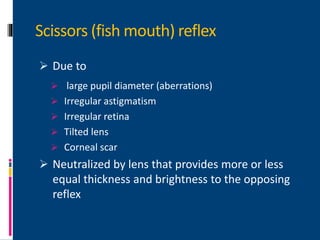
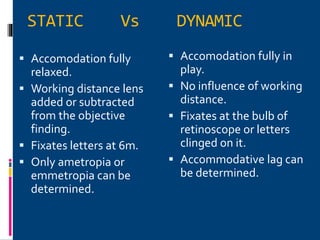


This presentation discusses retinoscopy, which is an objective method of determining refractive error by neutralizing the movement of light reflected from the retina. The history, theory, procedure, and types of retinoscopy are explained. Static retinoscopy finds the far point, while dynamic retinoscopy assesses accommodation. Observations of the retinoscopic reflex indicate refractive errors, and neutralization with lenses determines the prescription. Potential sources of error and techniques to confirm astigmatism are also reviewed.























































































