
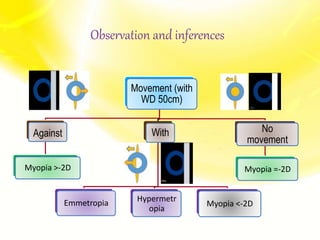
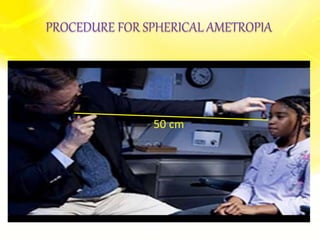
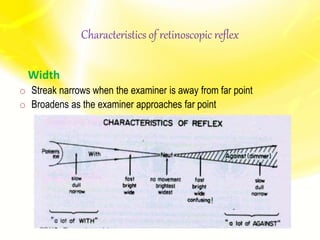
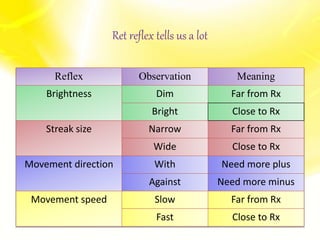

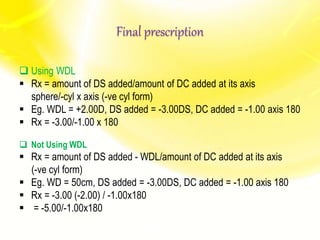
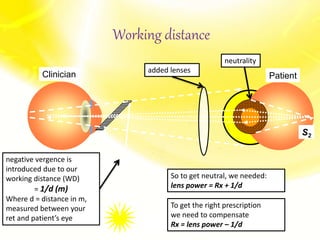


The document is a comprehensive presentation on retinoscopy, covering its application in diagnosing spherical ametropia and astigmatism, along with detailed explanations of various types of astigmatism. It outlines the procedures, techniques, and necessary equipment for performing retinoscopy, including the role of different lenses and the significance of retinoscopic reflex characteristics. Additionally, the document discusses troubleshooting common issues encountered during the procedure and the calculations for final prescriptions based on findings.




































































































