Downloaded 164 times
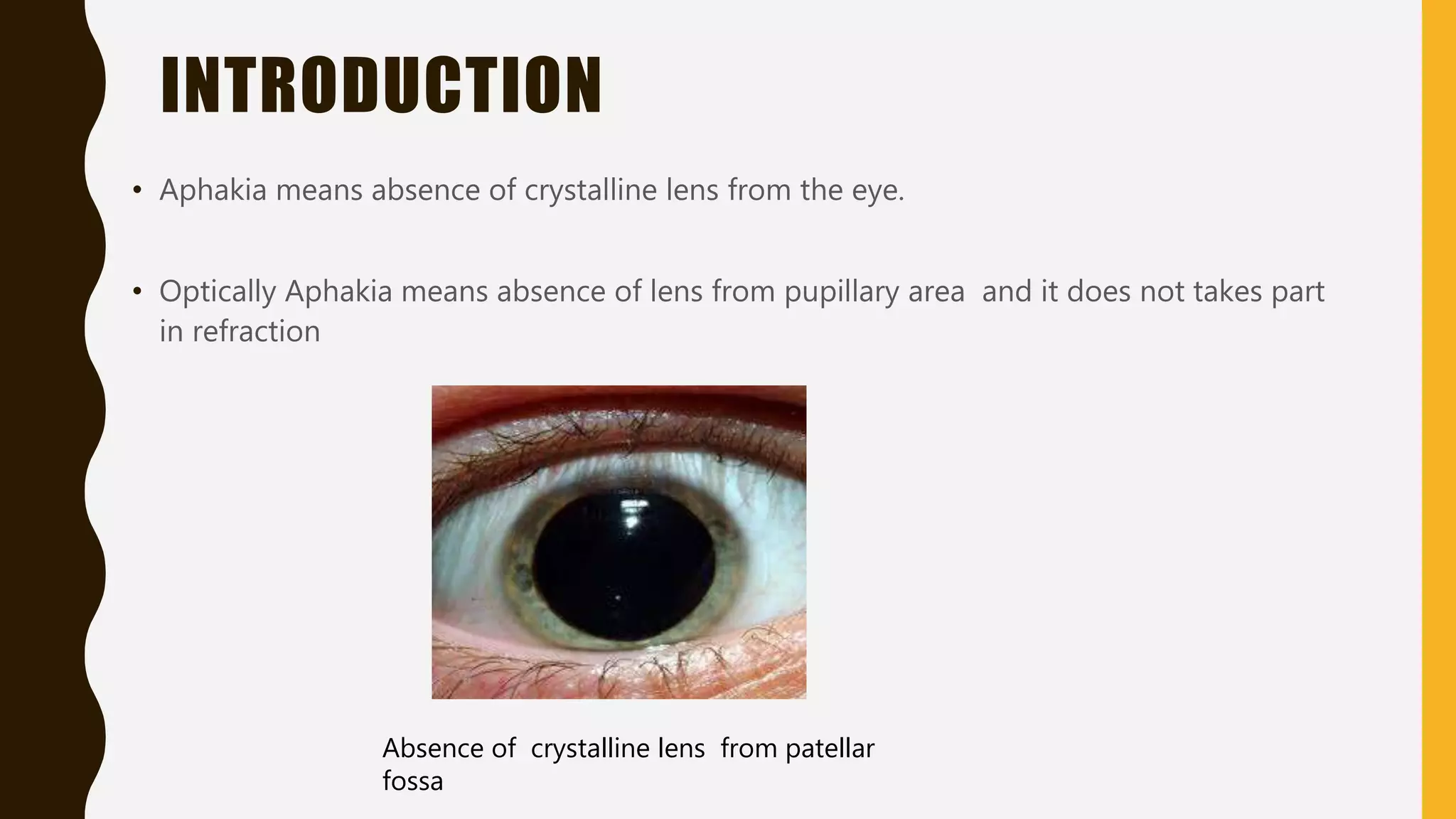
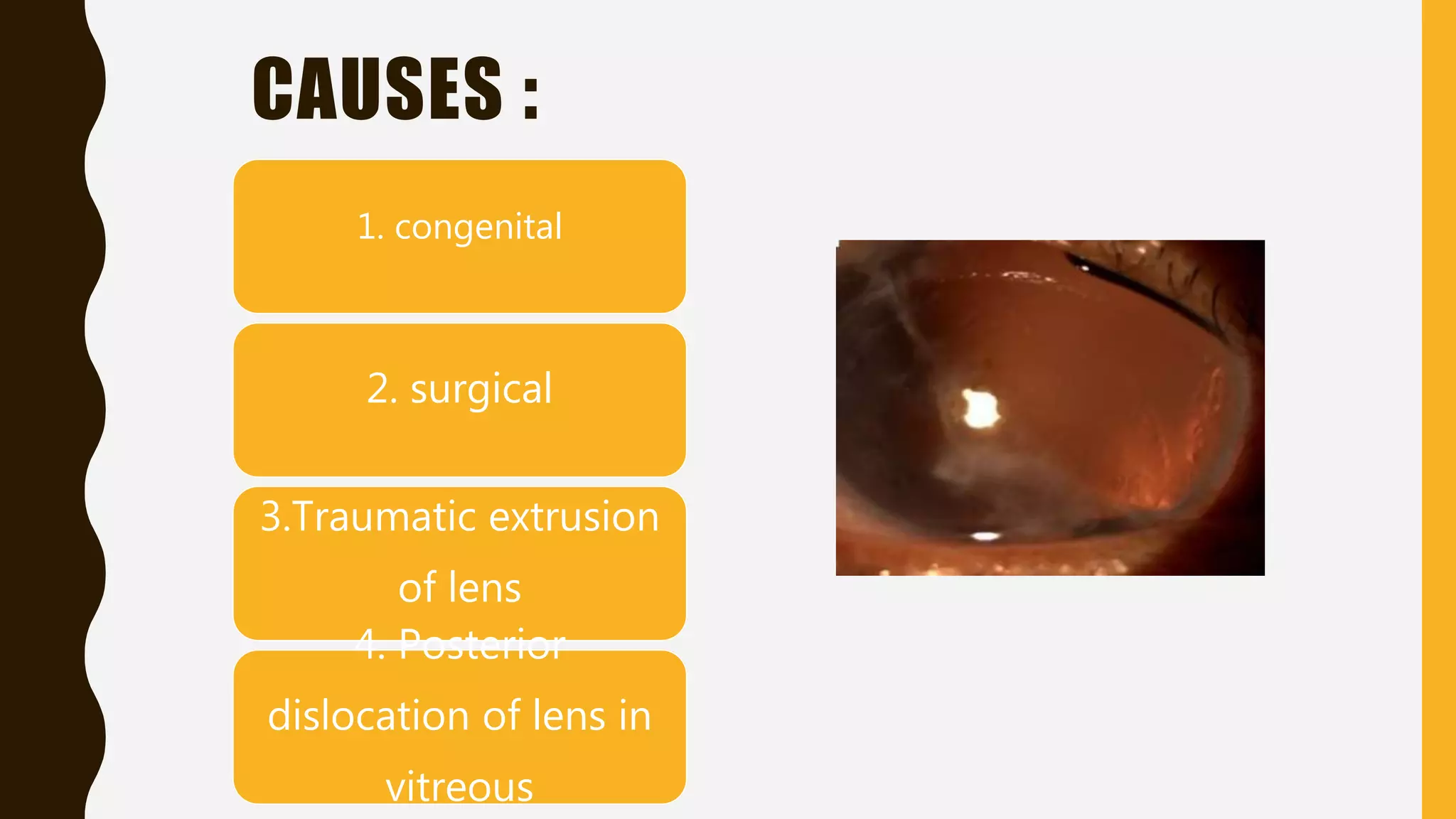

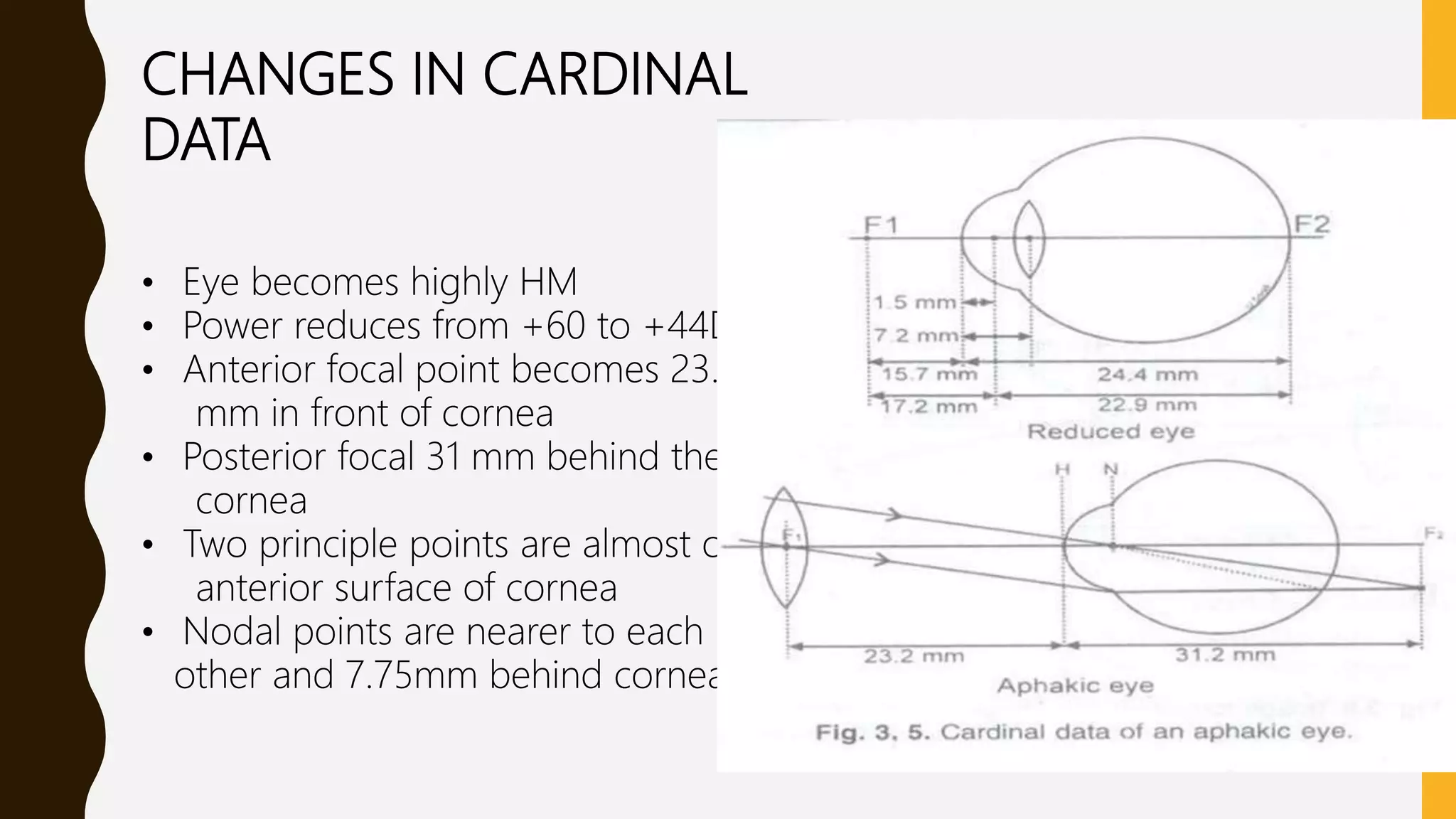
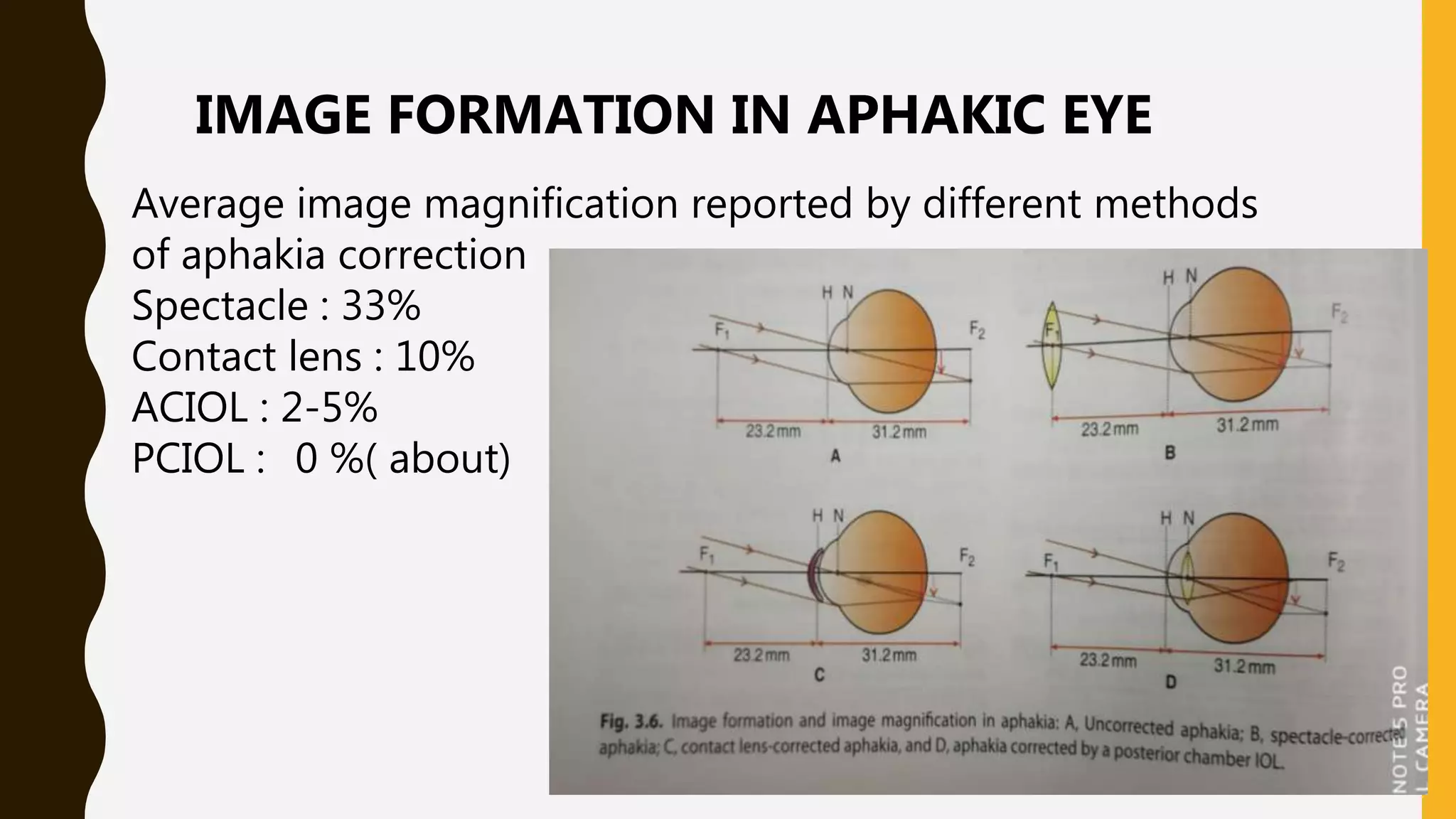

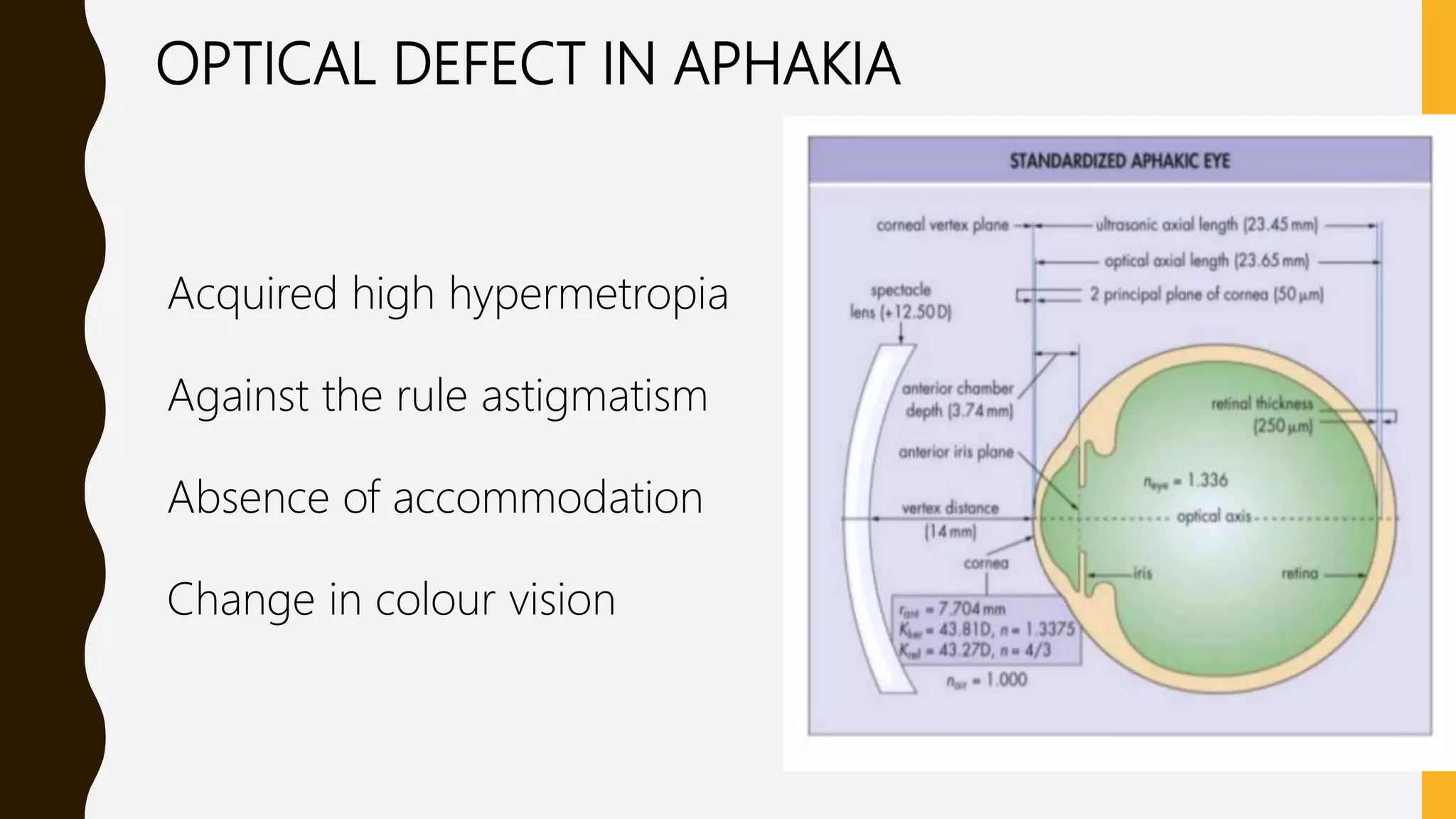





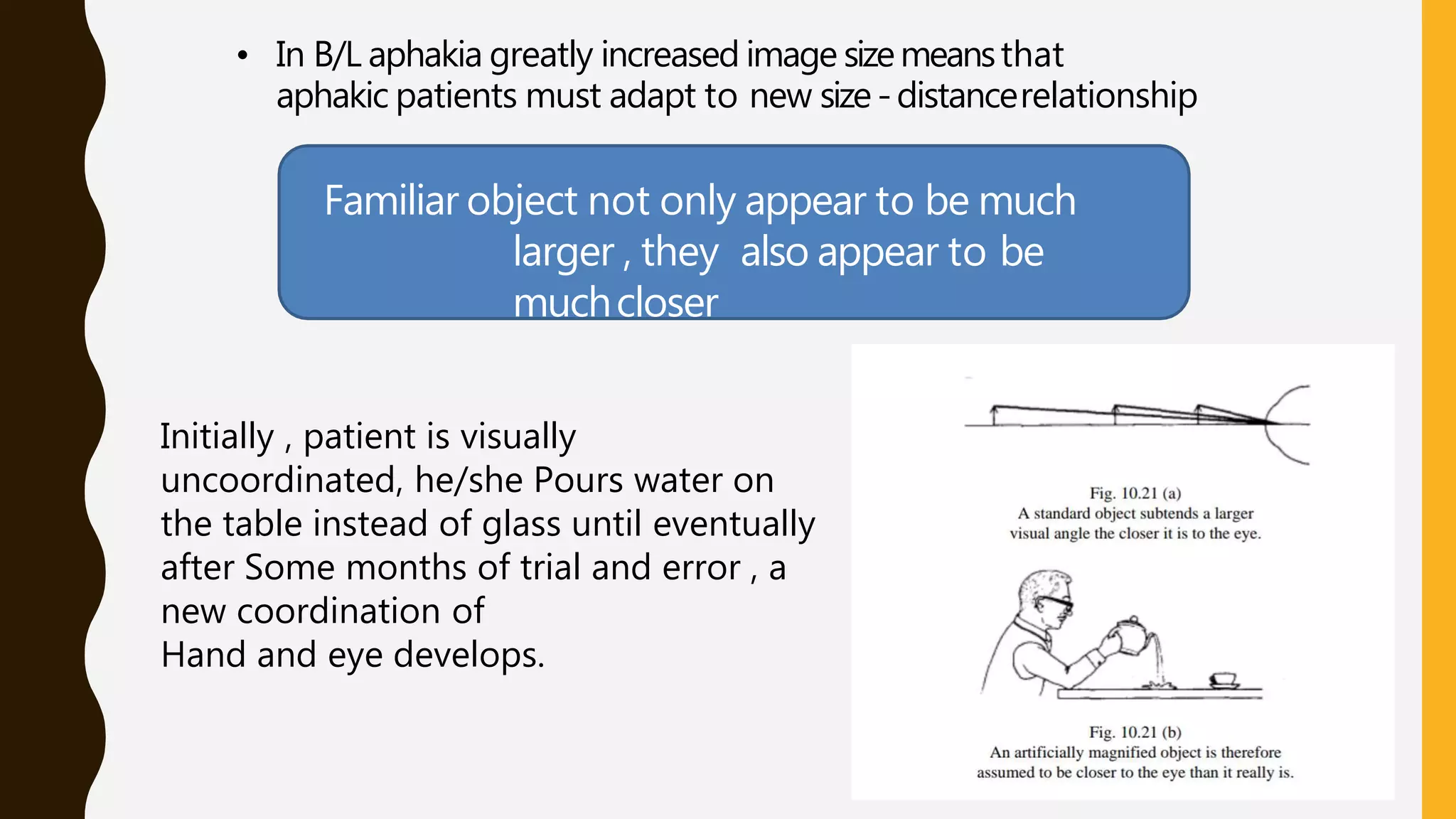

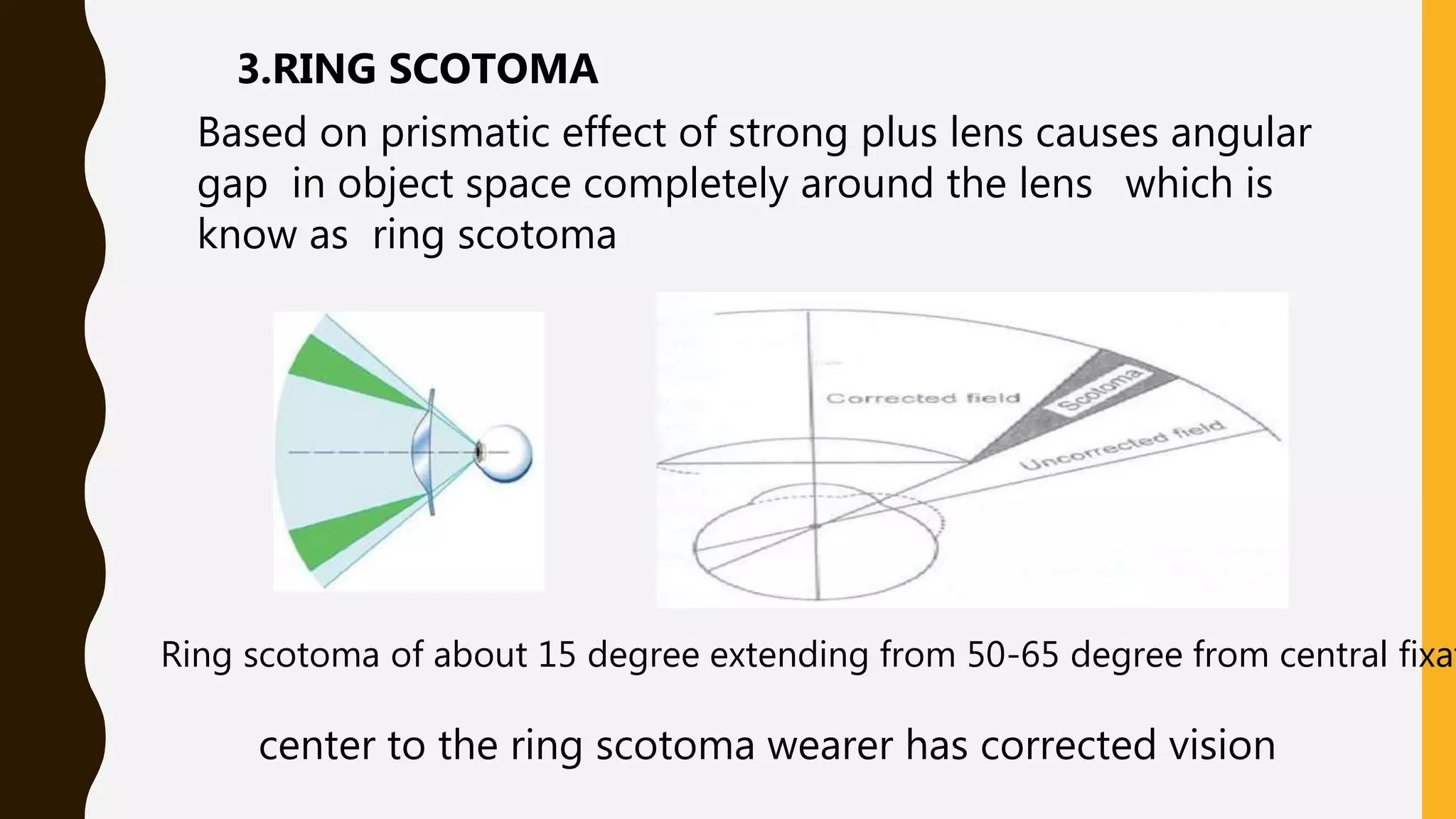
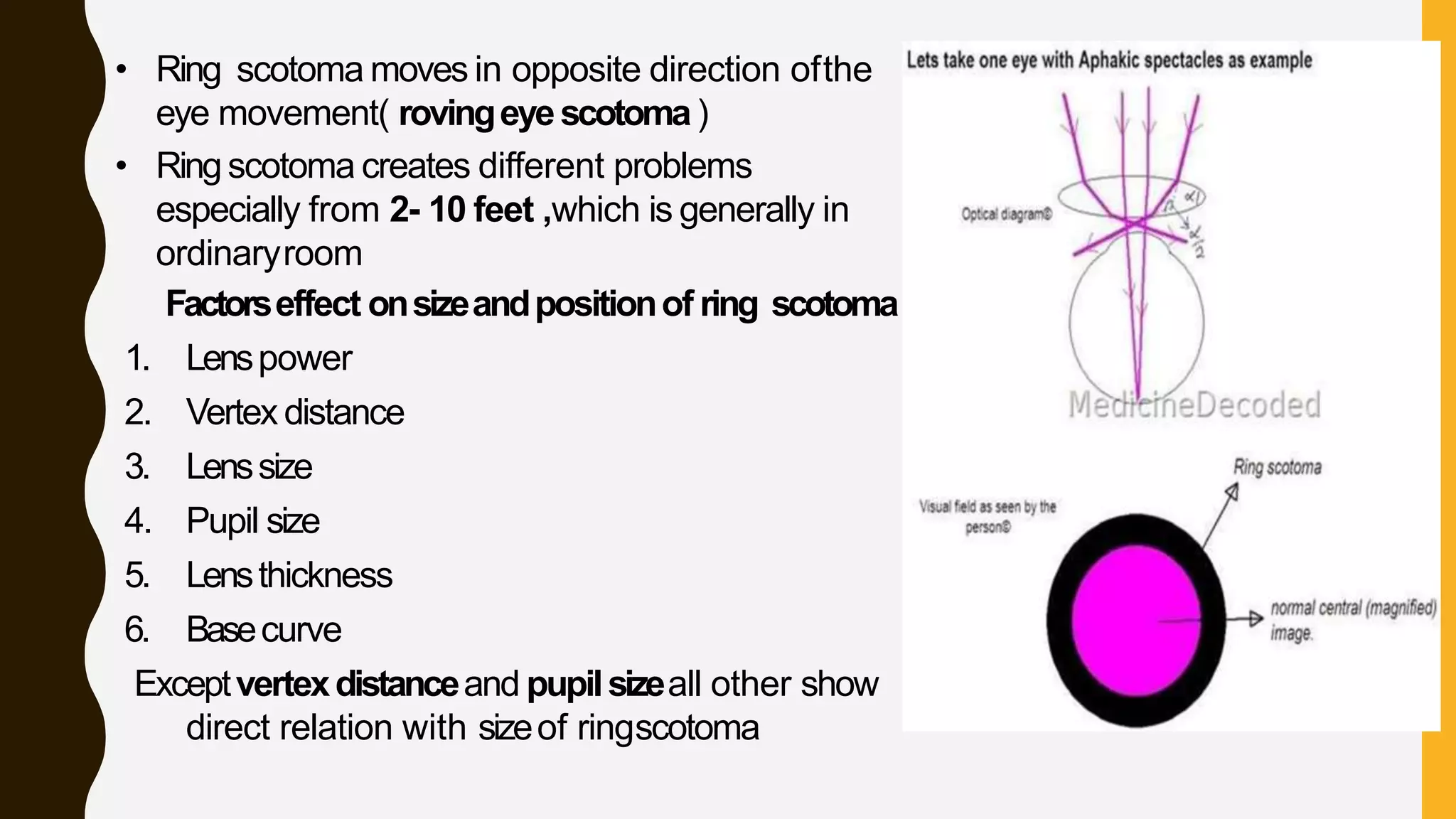
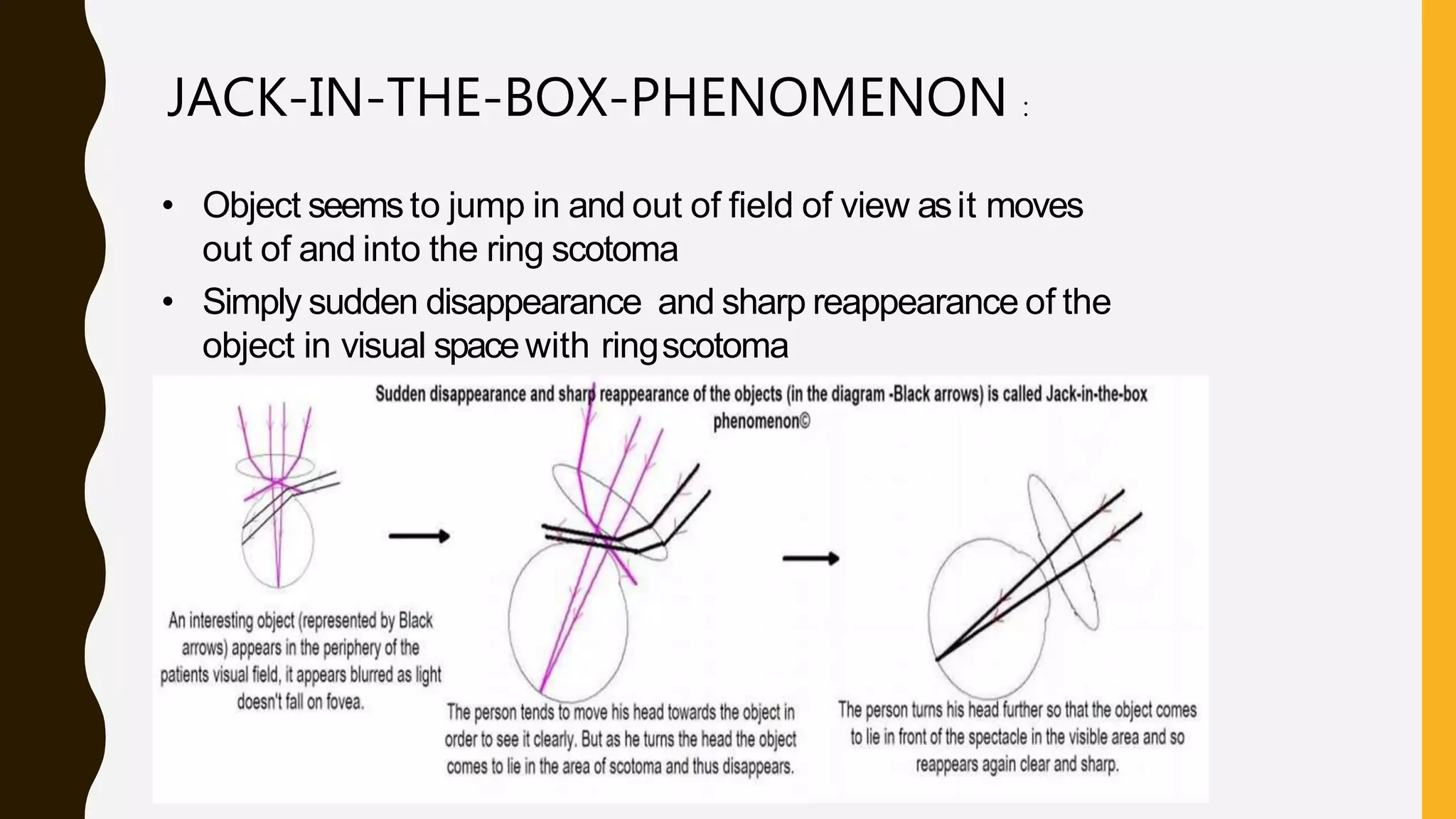

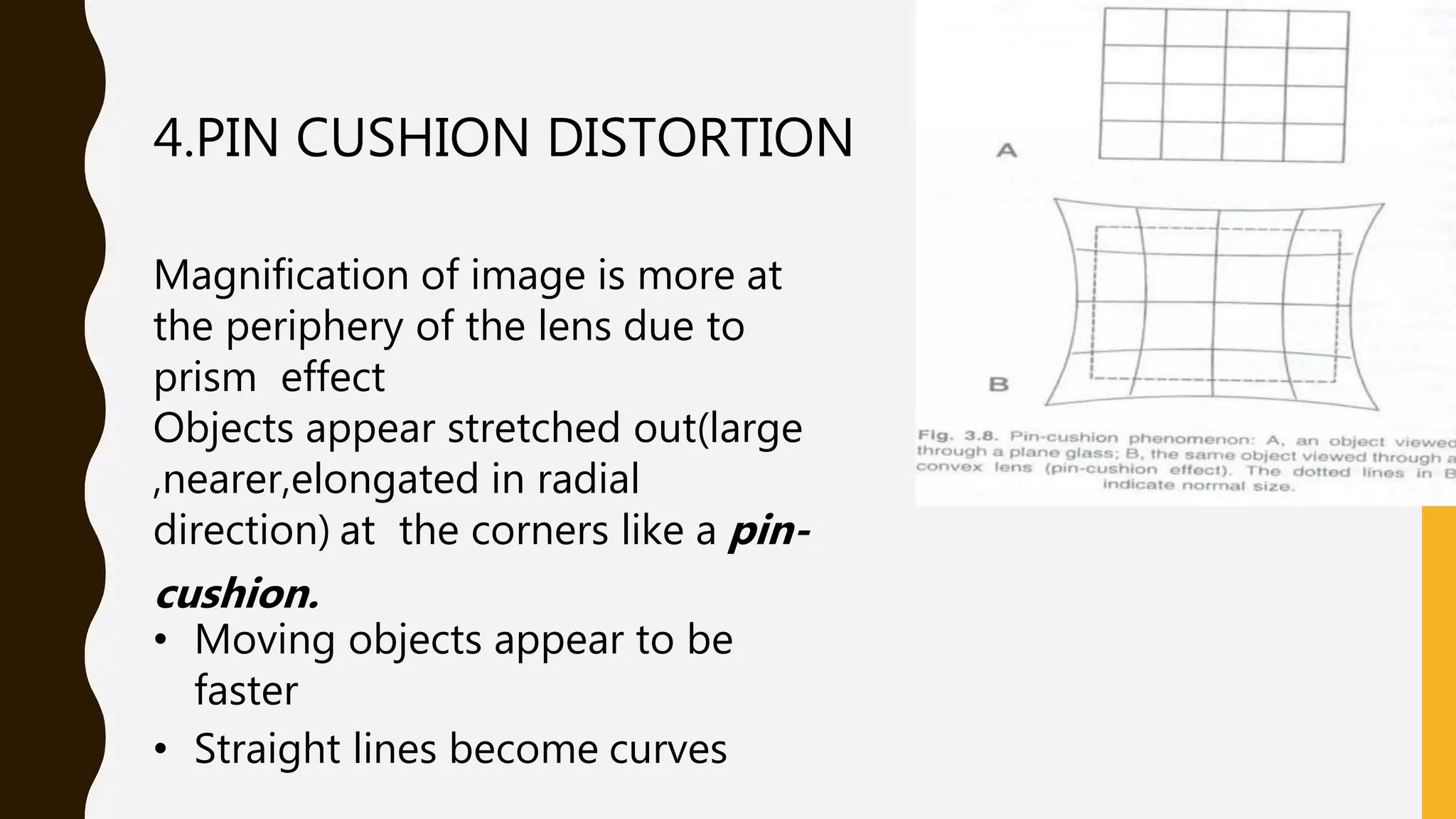










- Aphakia is the absence of the crystalline lens from the eye. It can be congenital or caused by surgery or trauma. - In aphakia, the eye becomes highly hyperopic, the anterior focal point moves forward, and the retinal image is magnified. This decreases visual acuity and field of view. - Aphakia is treated with spectacles, contact lenses, or intraocular lenses. Spectacles cause issues like increased image size, ring scotomas, and reduced field of view. Contact lenses and IOLs provide better image quality but have risks of complications.