Downloaded 360 times

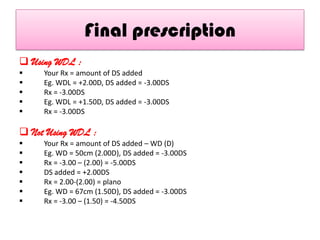
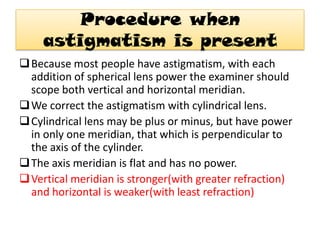
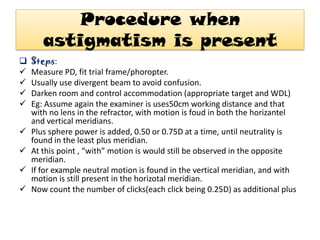
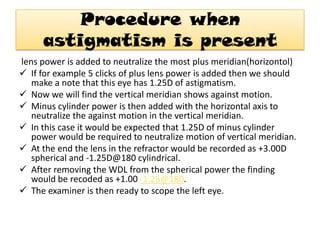


This document provides an overview of retinoscopy, including: - Retinoscopy is an objective technique to determine refractive errors by observing the movement of light reflected from the retina. - The practitioner modifies the movement of the reflected light with trial lenses to find the point of reversal and determine the refractive error. - It describes the parts of the retinoscope and how it works, as well as techniques for static and dynamic retinoscopy to evaluate spherical and cylindrical refractive errors. - The document outlines the procedure for retinoscopy, including controlling accommodation, adding trial lenses to find the point of neutralization or reversal, and determining the final refractive prescription.























































































