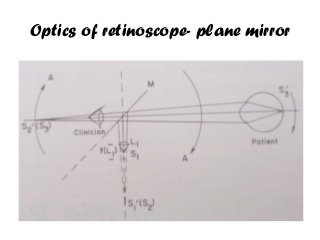
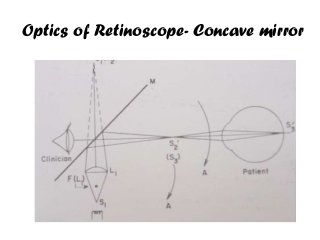
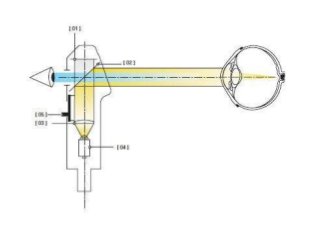
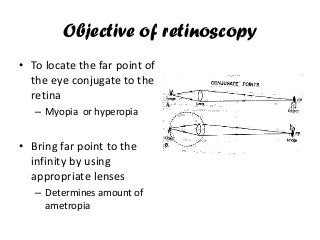
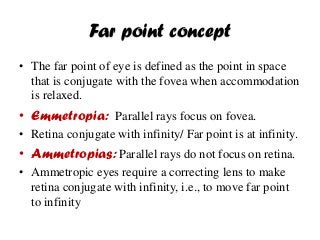
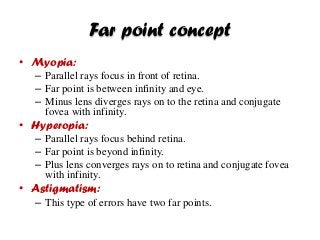


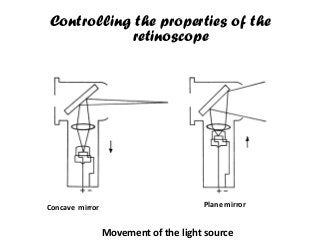
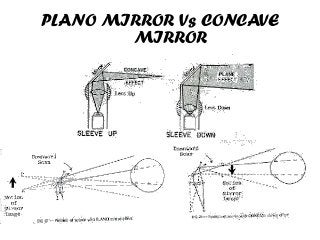
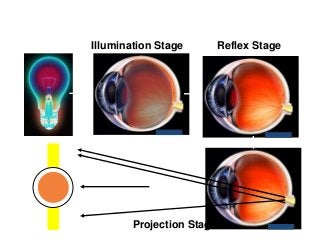
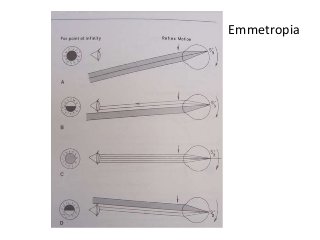
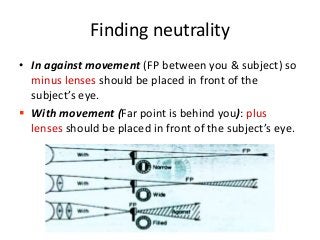
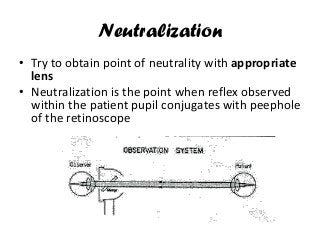
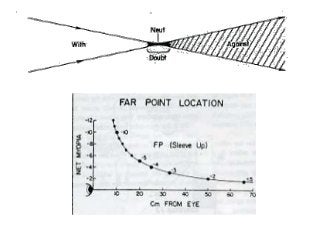
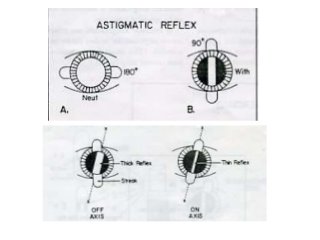
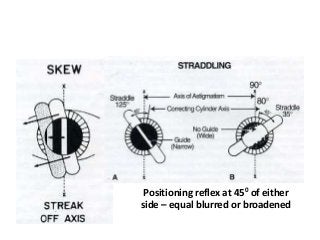
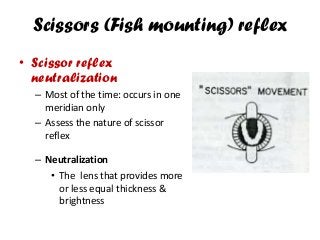


The document discusses the objective and procedure of retinoscopy, including the optics and use of the retinoscope to determine refractive errors by finding the neutralization point of the retinal reflex. It explains how static retinoscopy is performed by having the subject fixate at a distance while dynamic retinoscopy is done with fixation closer to the retinoscope. The document also outlines potential sources of error and techniques for dealing with spherical refractive errors as well as astigmatism.























































































