



















![Indications for cycloplegic refraction
• Symptom of ‘turning eye’
• Other suspicious symptom (e.g. young child closing or covering one
eye)
• Esotropia
• Significant esophoria
• Low accommodation
• Unstable objective or subjective refraction
• Large discrepancy between objective and subjective results
• Significant anisometropia in young child
• Spasm of the near triad [pickwell]](https://image.slidesharecdn.com/cycloplegicagentscyclorefraction-140403105845-phpapp01/85/Cycloplegic-agents-cyclorefraction-30-320.jpg)



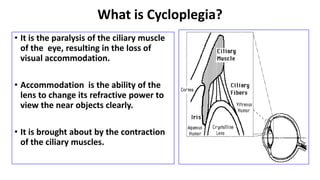
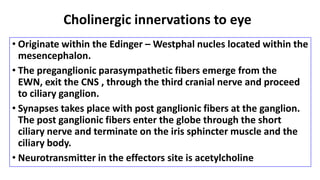
Cycloplegia is the paralysis of the ciliary muscle resulting in the loss of accommodation. Cycloplegic agents cause cycloplegia by blocking the muscarinic receptors in the eye. Cyclopentolate is commonly used for routine cycloplegic refraction in children and adults due to its fast onset and relatively short duration. Cycloplegic refraction is used to objectively determine refractive error when accommodation is paralyzed, and is indicated for young children with suspected latent hyperopia or accommodative esotropia. Cycloplegia is considered complete for refraction when a dilated pupil and no residual accommodation is detected via push-up test.