Downloaded 1,820 times
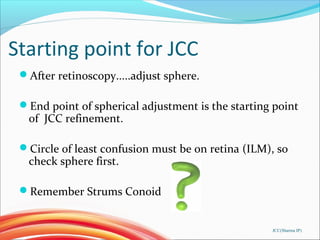
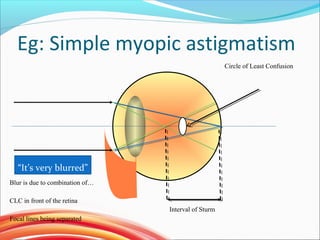
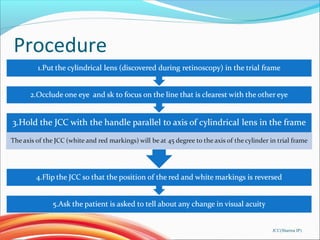
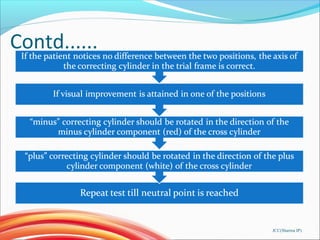
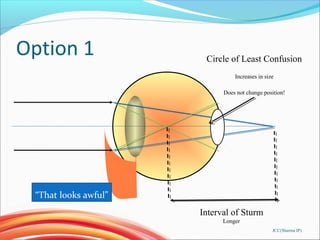
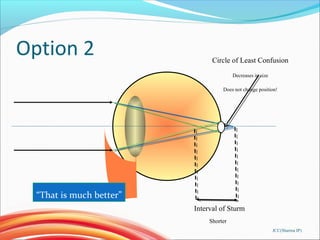
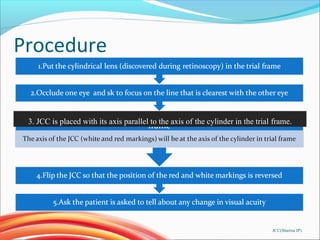
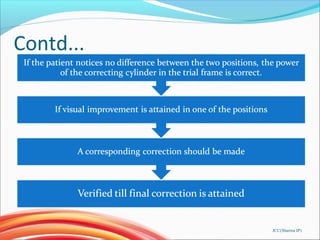




The document provides information about the Jackson Crossed-Cylinder (JCC) technique for determining astigmatism during eye exams. It discusses the optics and proper use of the JCC. It describes the historical origins of the JCC, how it works, and the step-by-step procedure for using it to refine the axis and power of astigmatic corrections. Common sources of error are also outlined. The JCC is presented as an important tool for optometrists to accurately measure and correct astigmatism in clinical practice.








































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)








