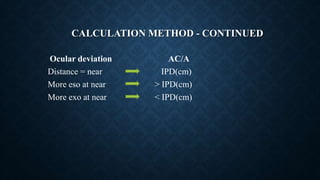
This document discusses the AC/A ratio, which is the ratio of accommodative convergence to accommodation. It defines the AC/A ratio and notes the normal range is 3-5 prism diopters per diopter of accommodation. Abnormal AC/A ratios can cause strabismus. The document outlines methods to measure the AC/A ratio clinically and discusses its uses in diagnosing different types of strabismus and their management approaches.



![CALCULATED AC/A RATIO
AC/A = IPD +[N - D¹] / D
Where,
IPD = interpupillary distance in centimetres
N = near fixation distance in meters
D¹= near phoria (eso is plus and exo is minus)
D = far phoria (eso is plus and exo is minus)](https://image.slidesharecdn.com/acarationew-220209180507/85/Ac-a-ratio-9-320.jpg)