Download as PDF, PPTX
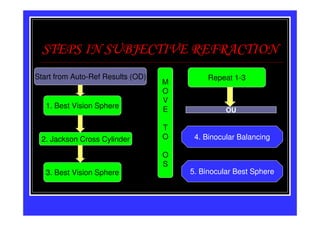
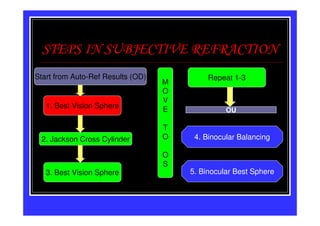
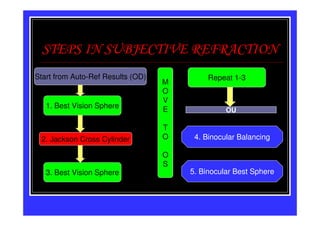
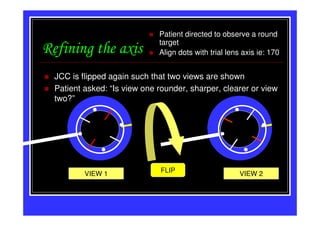
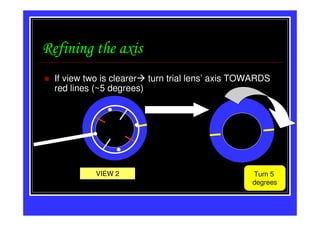
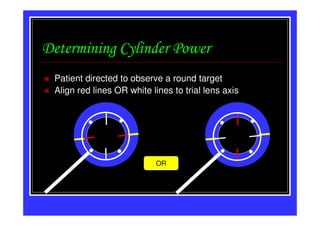
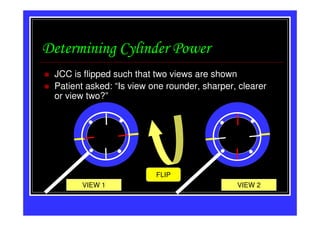
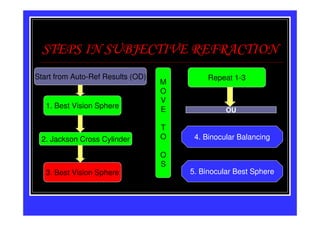
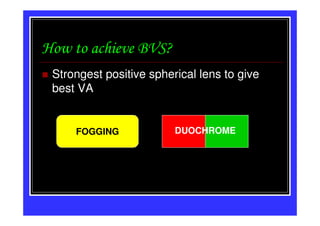
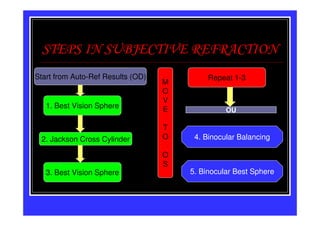
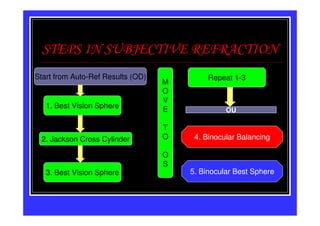
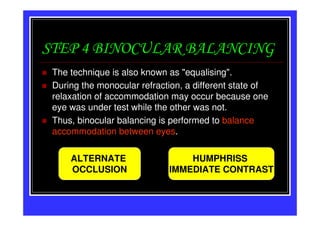
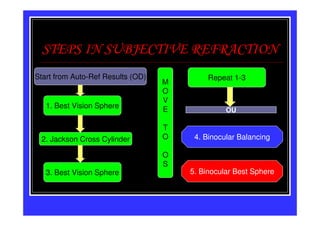
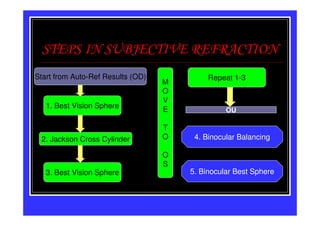
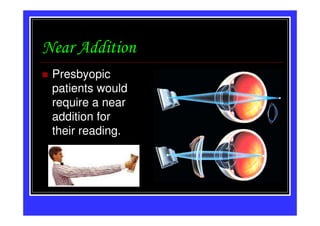
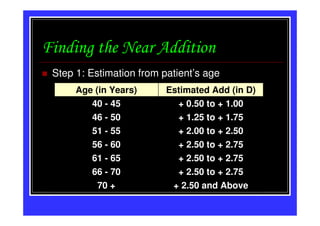
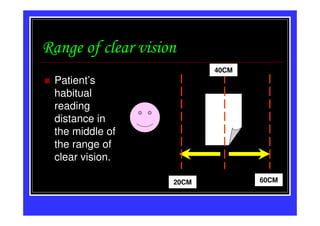
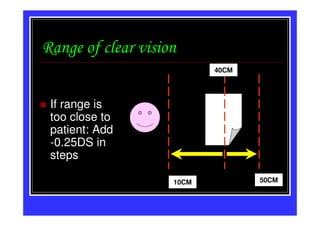
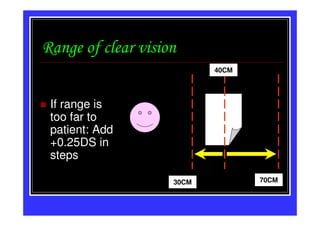
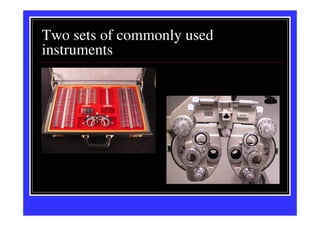

This document discusses the process of subjective refraction to determine a patient's prescription. It involves 5 main steps: 1) determining the best vision sphere for each eye, 2) using a Jackson Cross Cylinder to find the cylindrical axis and power, 3) refining the results, 4) binocular balancing to account for any differences between the eyes, and 5) determining the binocular best sphere. Fogging and duochrome tests are used to achieve the best vision sphere. Near additions are also considered for presbyopic patients based on their habitual reading distance and age. Trial lens sets and phoropters are the main instruments used.























































































