Downloaded 325 times

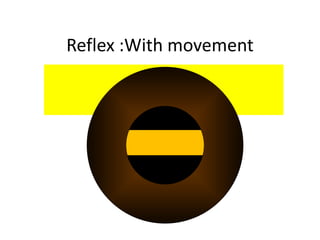
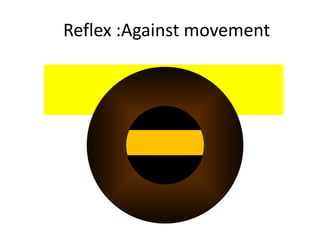
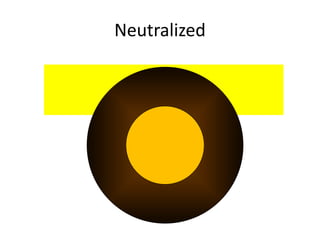
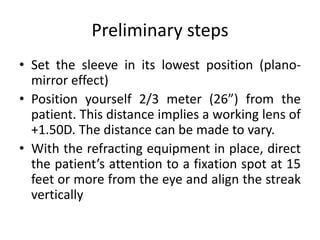


Retinoscopy is an objective method for measuring the optical power of the eye, illuminating the retina to observe the reflected light and assess refractive errors. The evolution of the technique includes key developments and contributions from various ophthalmologists, culminating in the modern retinoscope that incorporates advanced features for improved accuracy. The document details the practical application of retinoscopy, including handling techniques, error determination, and evaluating refractive states like myopia and hyperopia.











































































