Downloaded 99 times


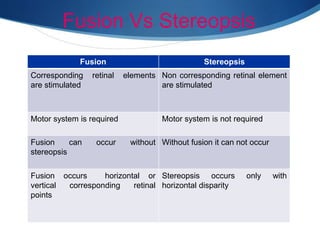
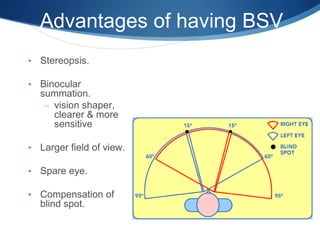








This document provides an introduction to binocular single vision (BSV) including its definition, grades, advantages, development, mechanisms, anomalies, and investigations. BSV is the coordinated use of both eyes to see a single image through the process of fusion. It develops in early childhood as the visual axes align and fusional movements are established. Maintaining BSV provides advantages like stereopsis and binocular summation. Investigations of BSV assess fusion, retinal correspondence, suppression, and stereopsis.























































































