Downloaded 494 times

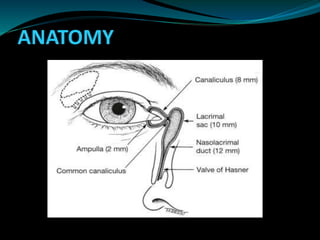
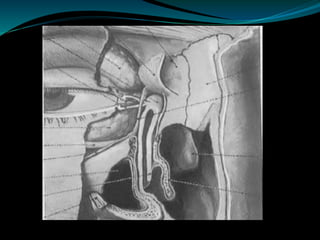
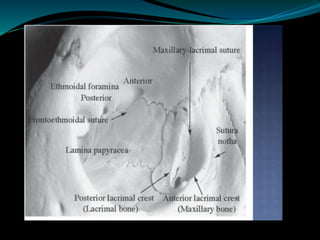




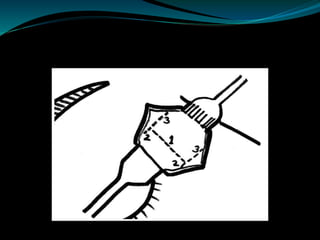


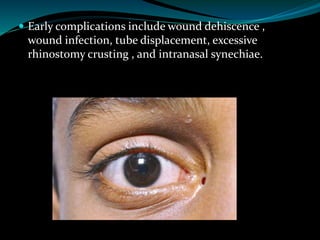
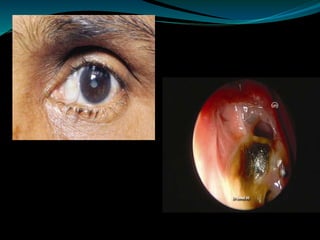
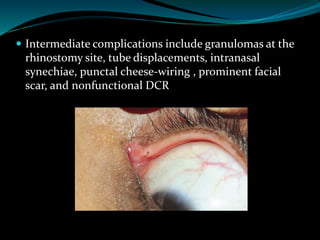
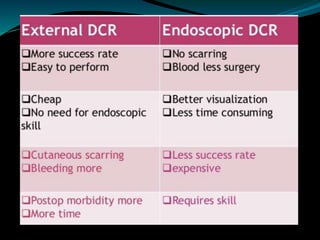


This document describes different surgical procedures for lacrimal sac obstructions, including dacryocystorhinostomy (DCR) and dacryocystectomy. It outlines the anatomy, indications, preoperative requirements, steps of conventional DCR including osteotomy of the lacrimal bone and suturing of nasal and sac flaps, and post-operative care. It also discusses endoscopic and endolaser techniques for DCR and the indications for dacryocystectomy. Complications of DCR include wound infections, synechiae formation, and osteotomy stenosis leading to procedure failure.























































































