Downloaded 473 times
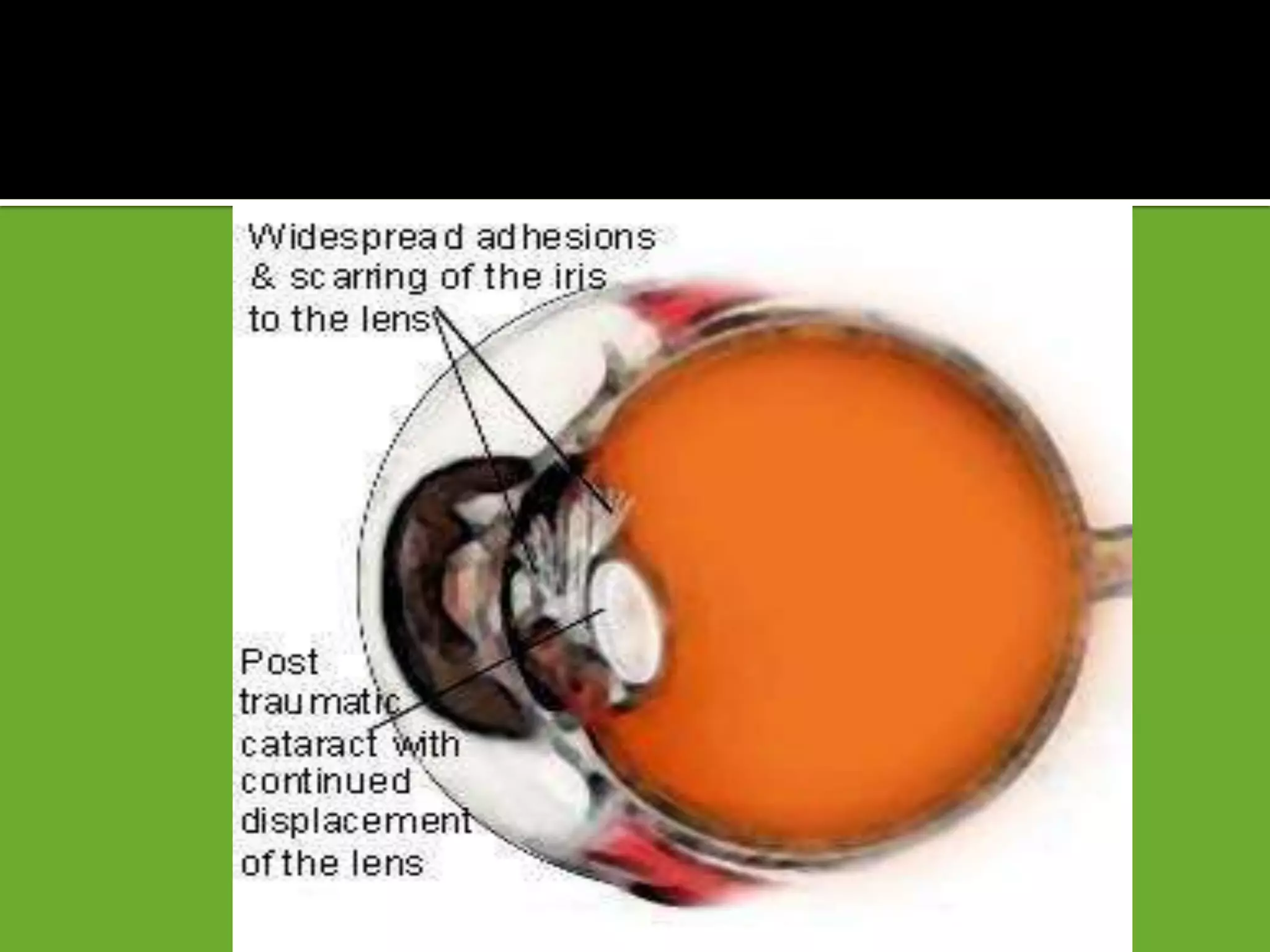
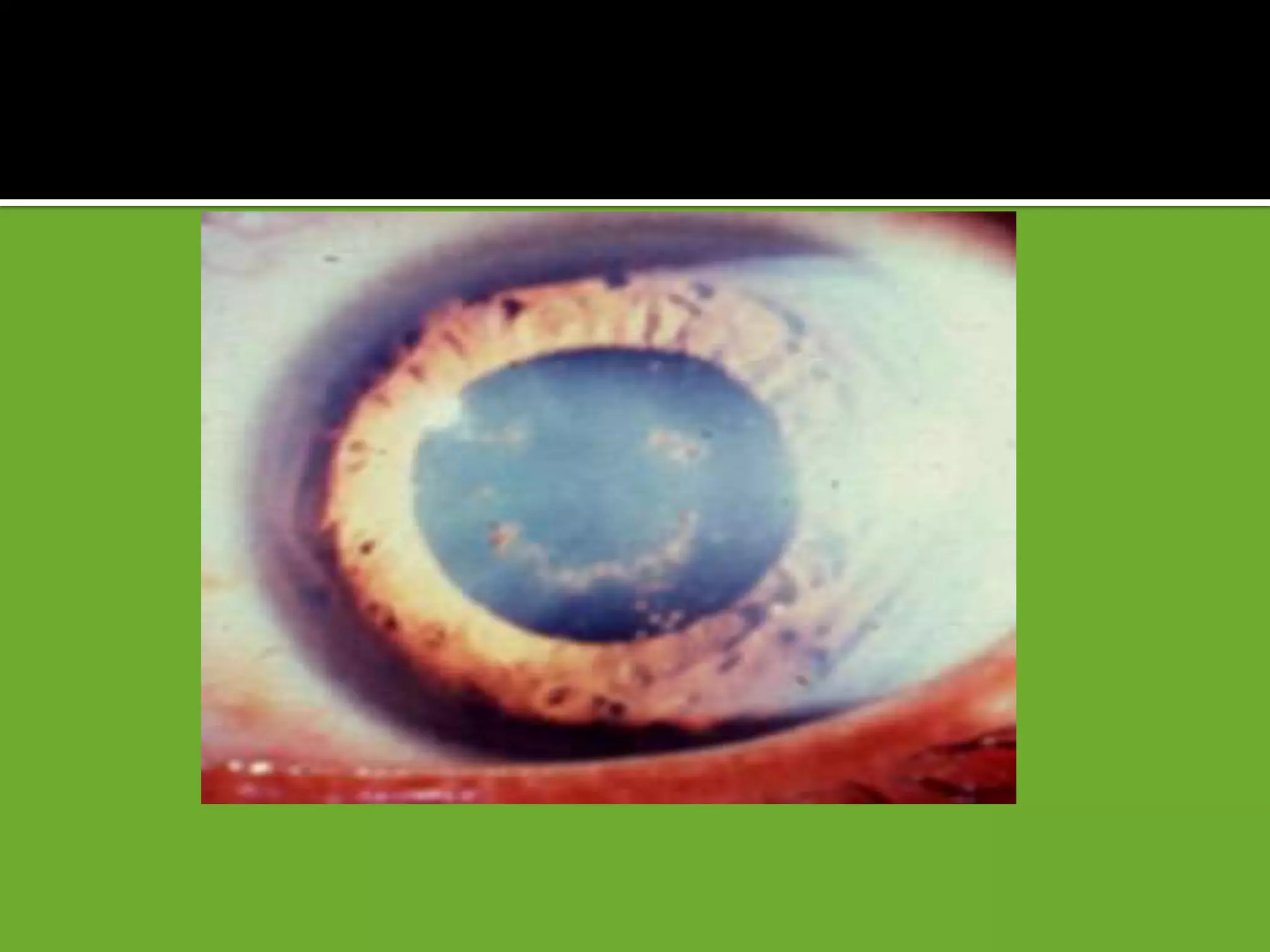
![ A ring-shaped anterior subcapsular opacity may underlie a Vossius
ring [. Imprinting of iris pigment on anterior lens capsule]
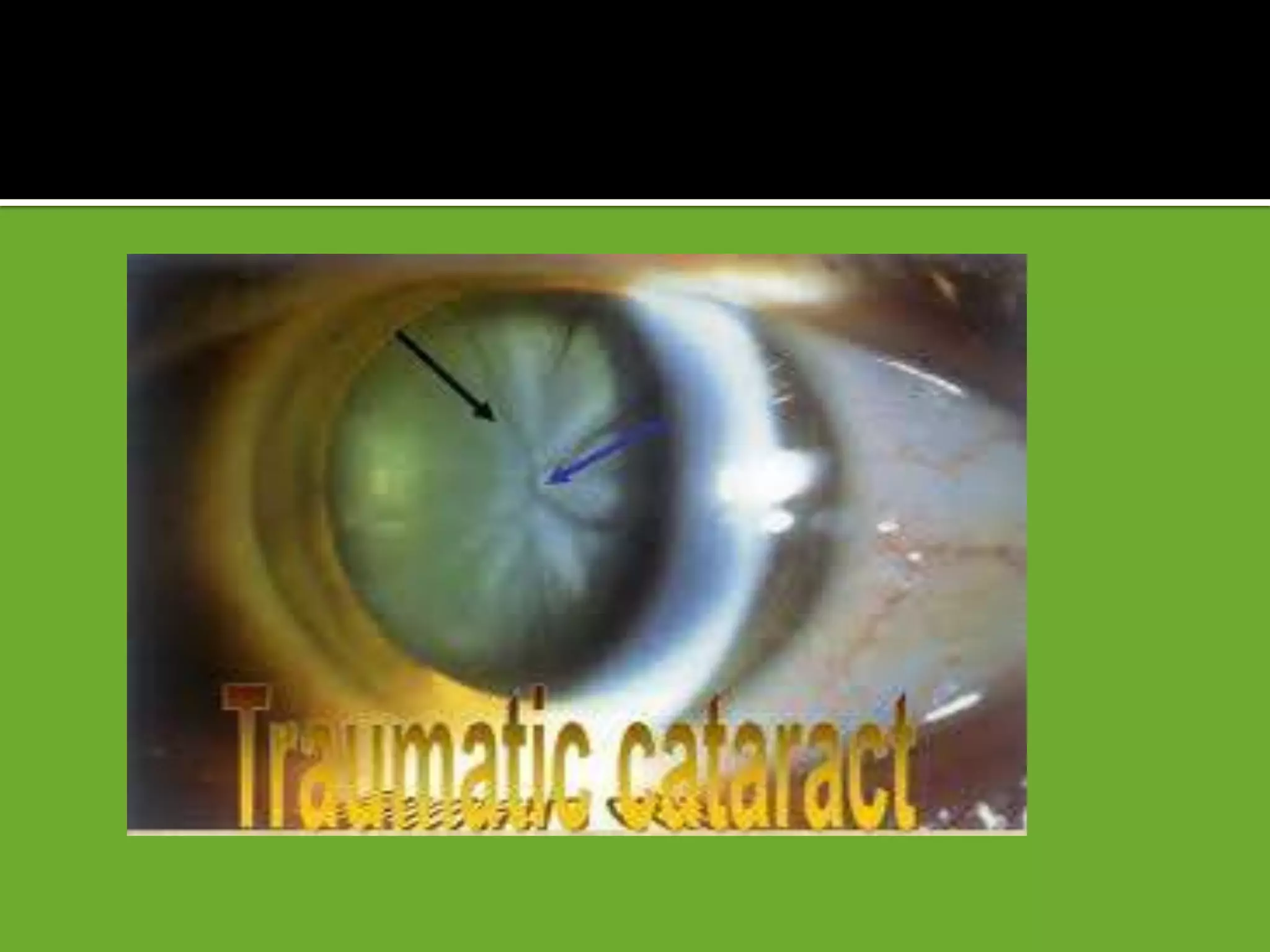
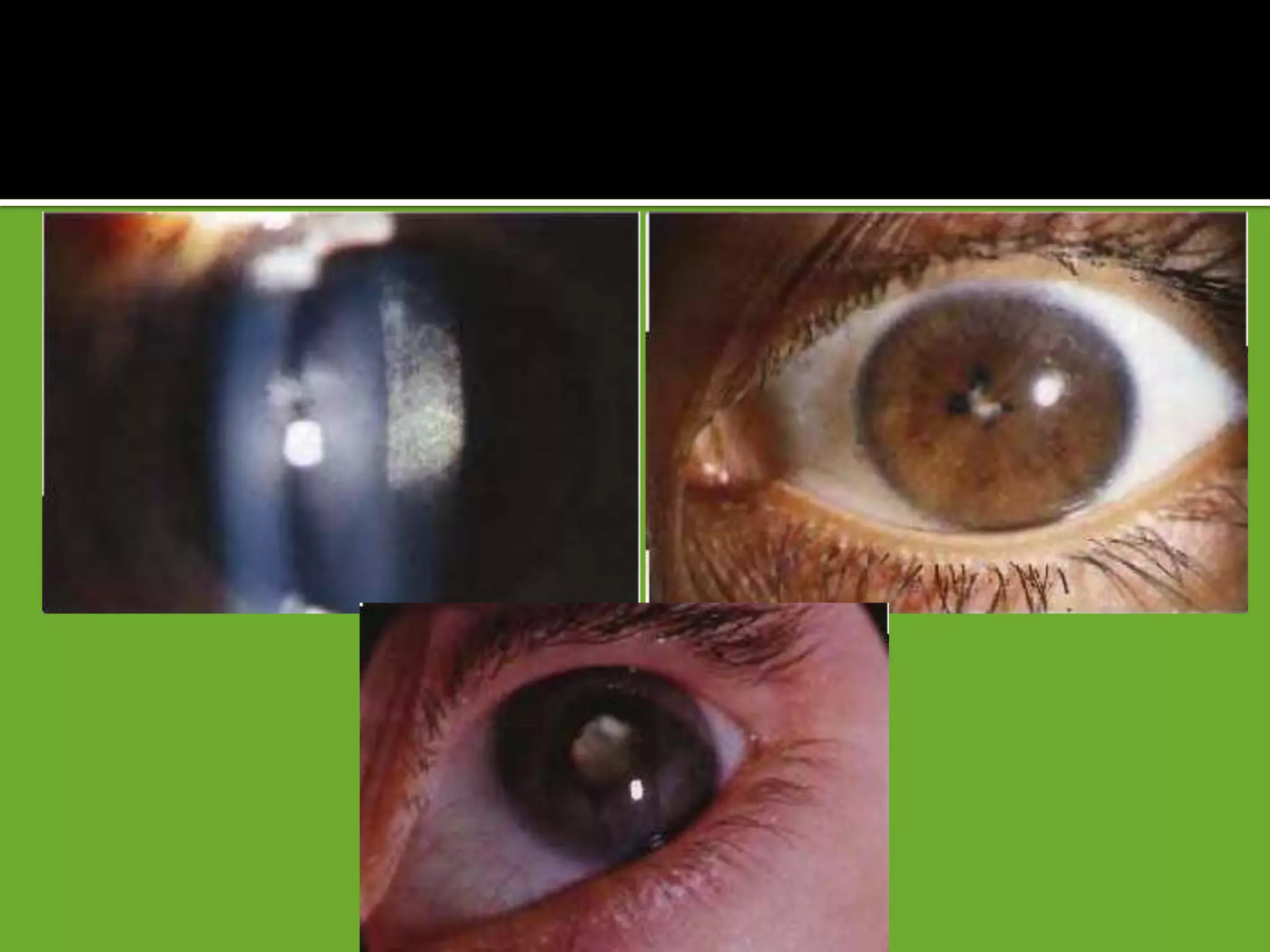
Commonly opacification occurs in the posterior subcapsular
cortex along the posterior sutures, resulting in flower -shaped opacity
[rossette] which may subsequently disappear, remain stationary or
progress to maturity.
Cataract surgery may be necessary for visually significant opacity.
Lens protein leak can lead to secondary Glaucoma,uveitis.](https://image.slidesharecdn.com/traumaticandcomplicatedcataract-130613205538-phpapp01/75/Traumatic-and-complicated-cataract-8-2048.jpg)
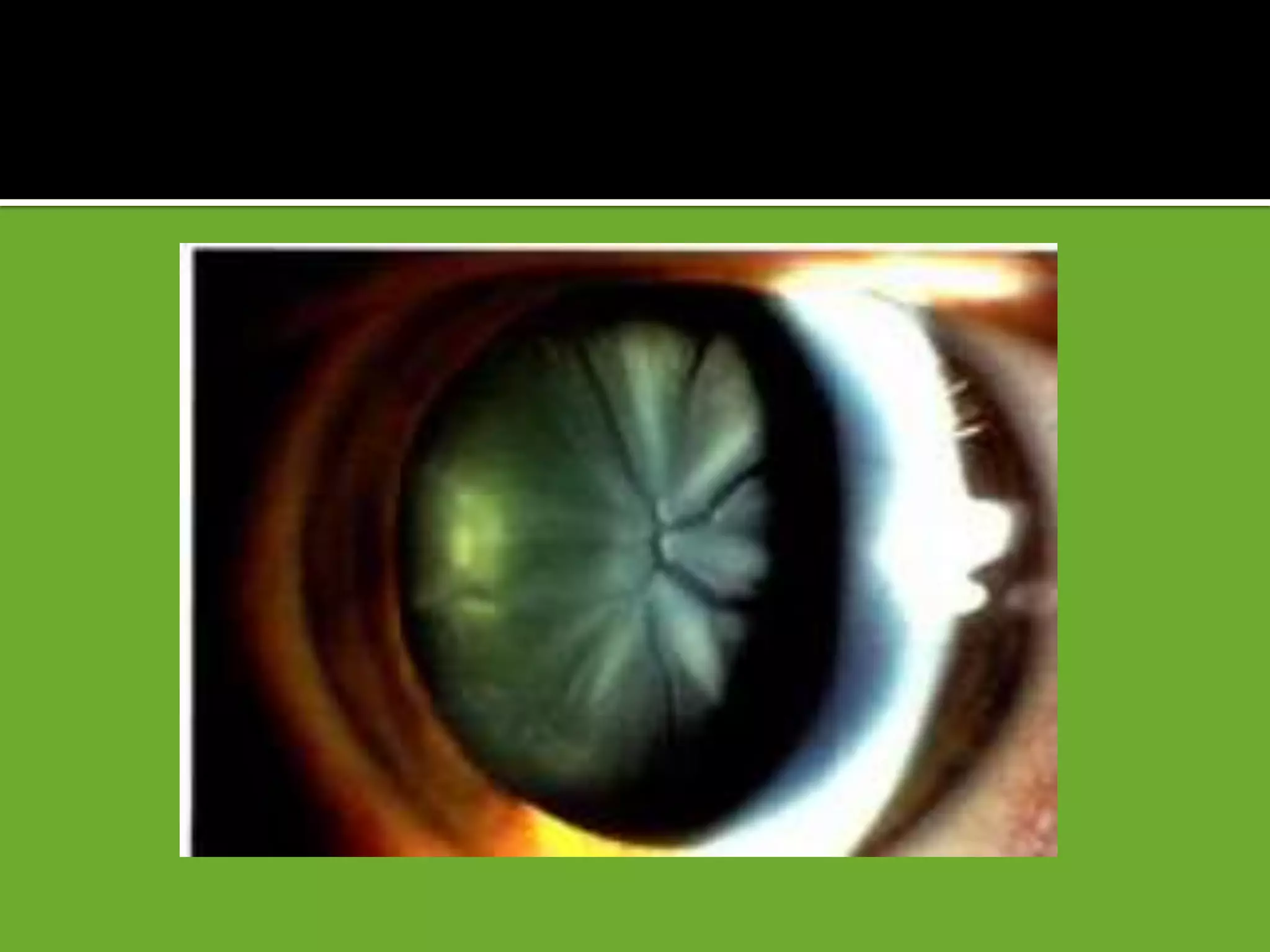


Cataract formation is commonly caused by blunt trauma to the eye and can result in flower-shaped opacities in the lens. Subluxation or dislocation of the lens may also occur due to trauma tearing the suspensory ligament. A cataract surgery may be needed to remove a visually significant cataract caused by trauma or other conditions like uveitis. Special considerations for surgery include damage to other ocular tissues, retained foreign bodies, inflammation, and zonular dehiscence.























































































