Download to read offline
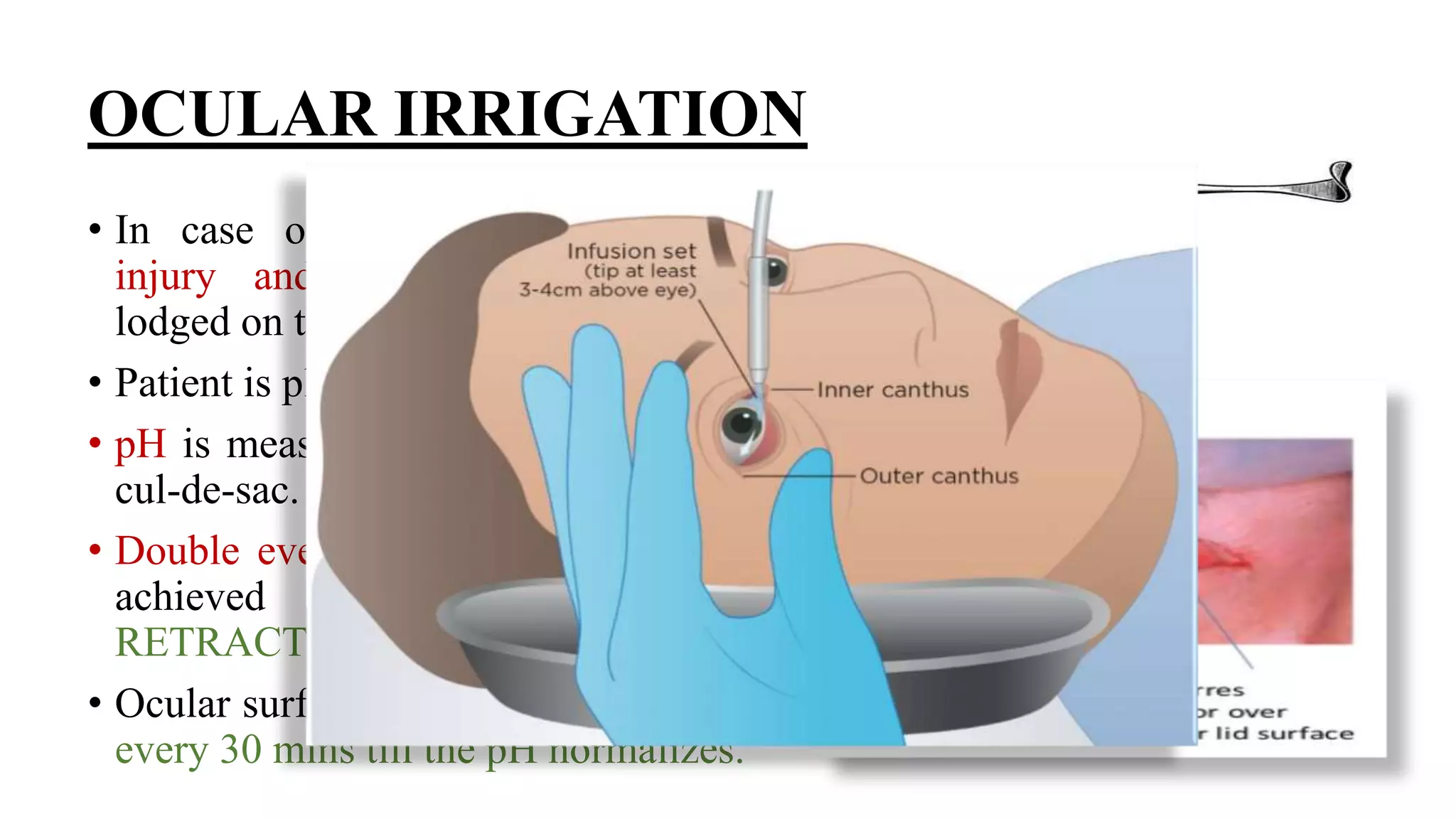


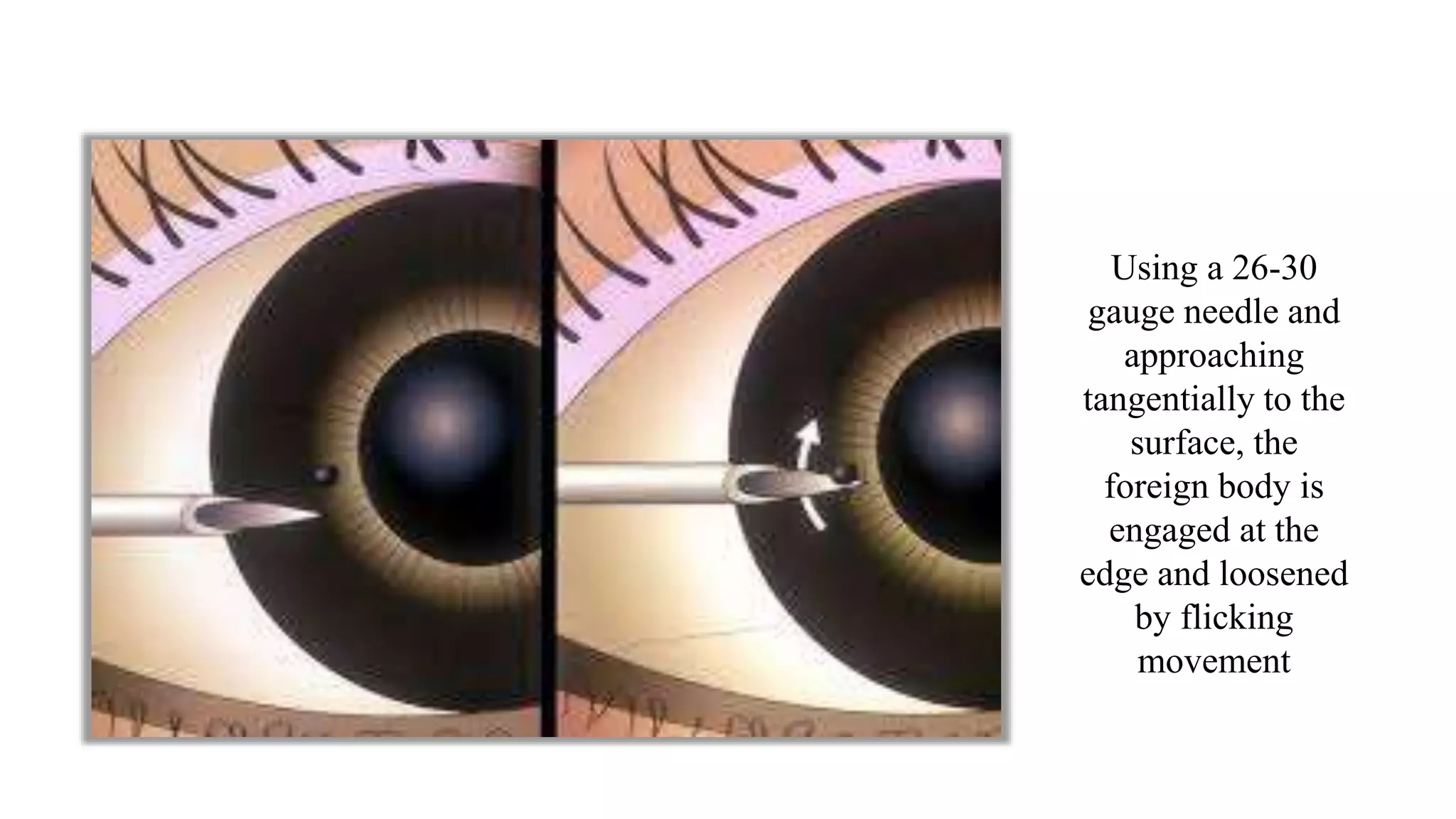
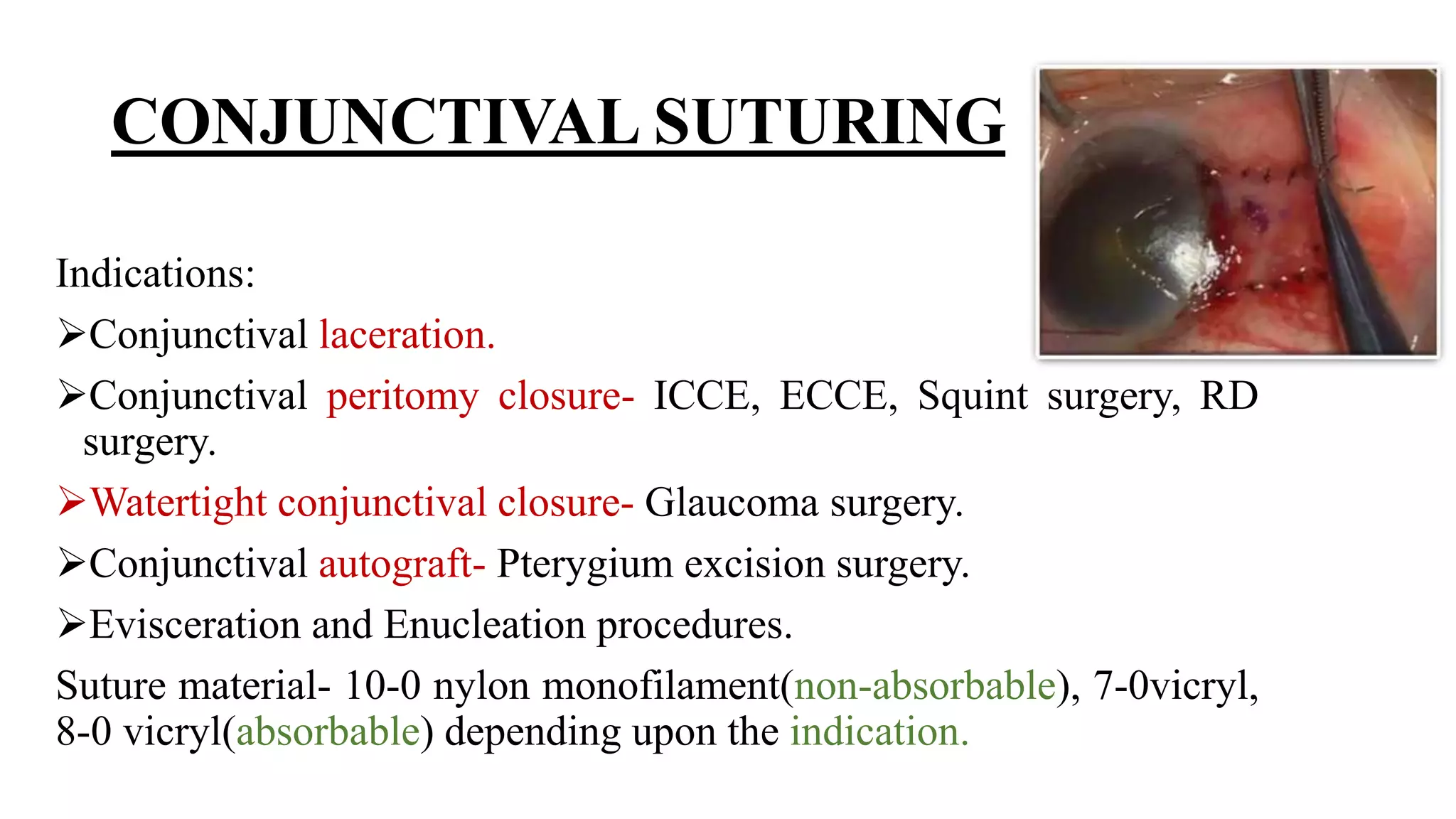
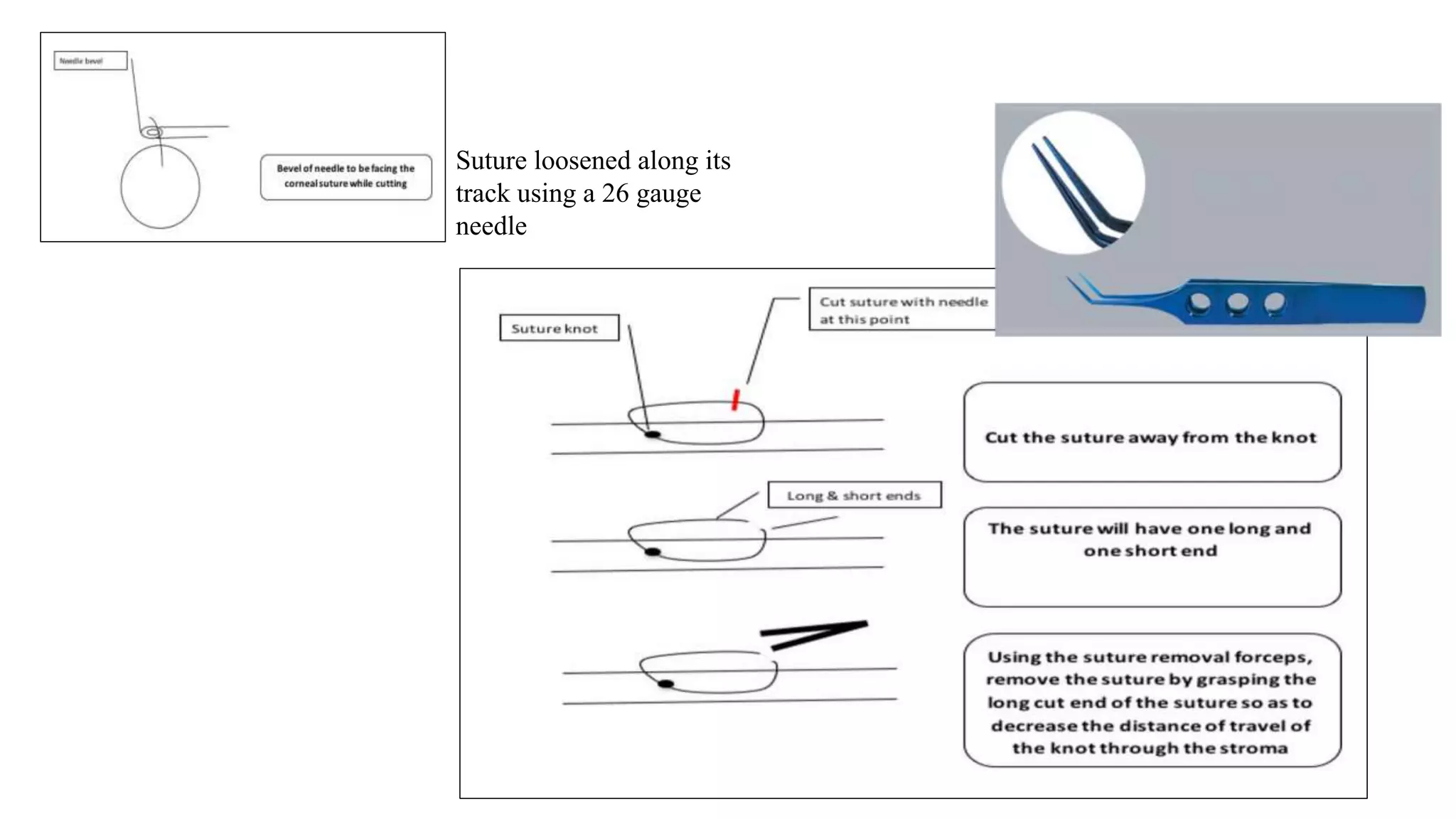
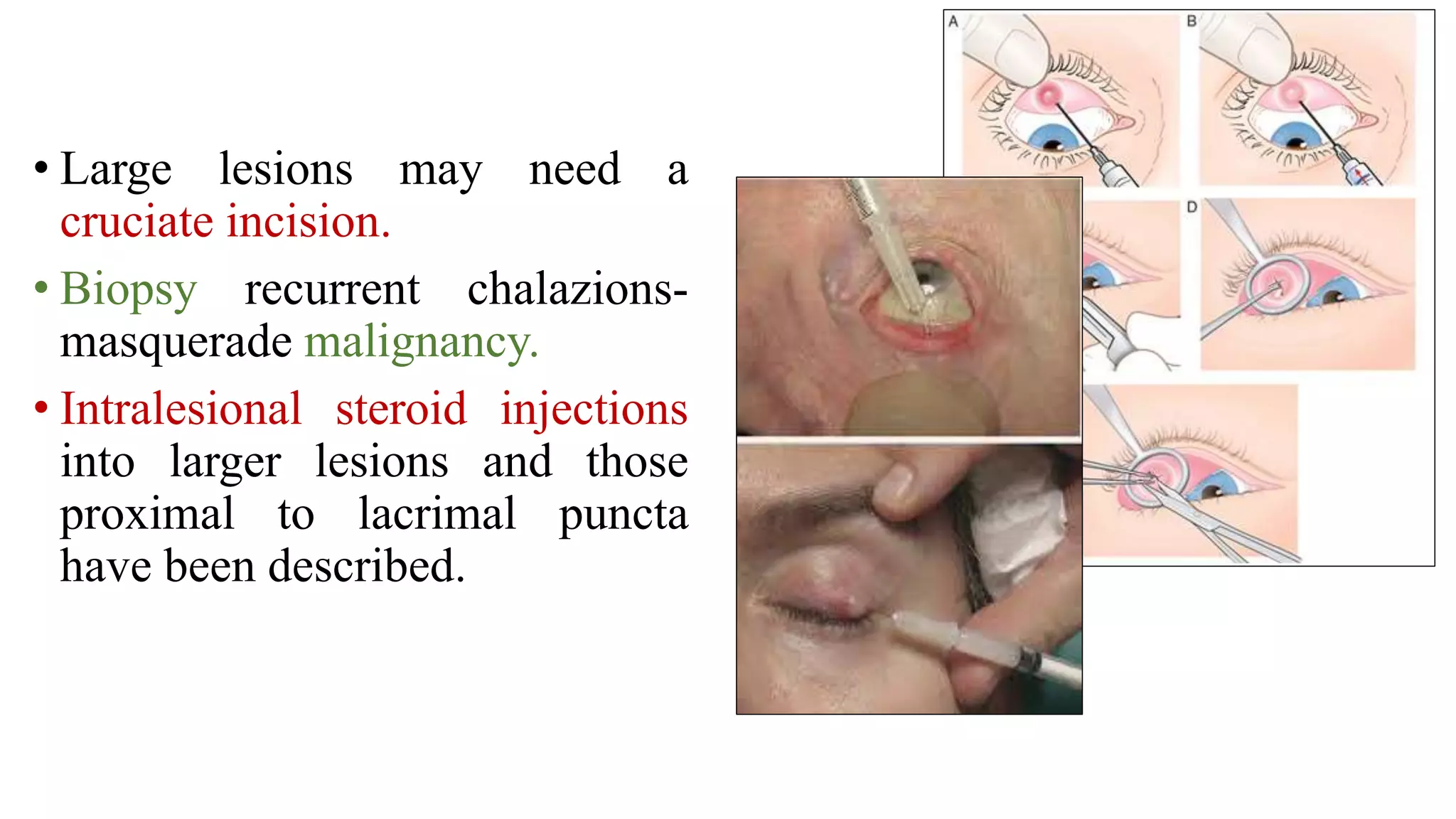
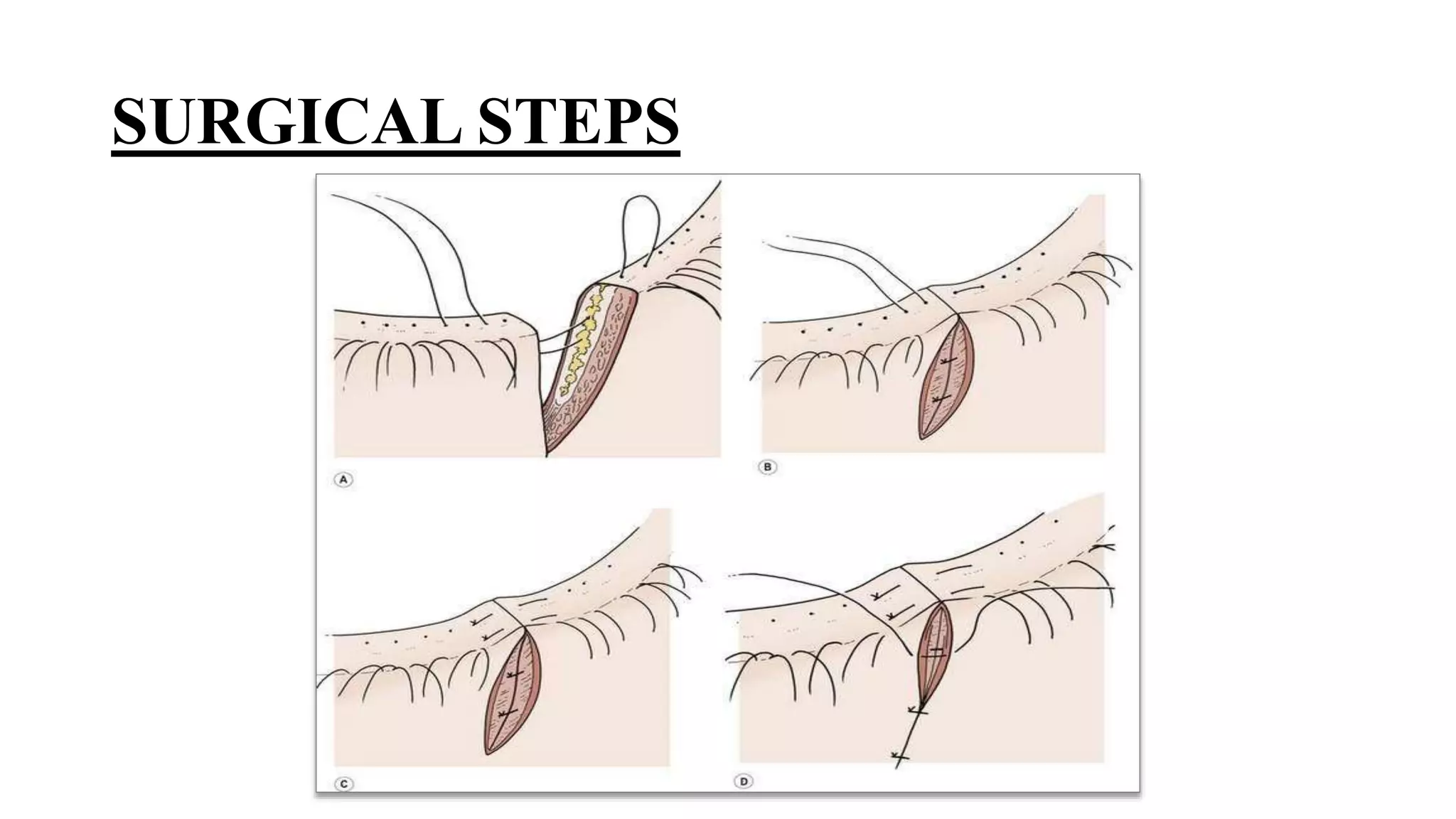
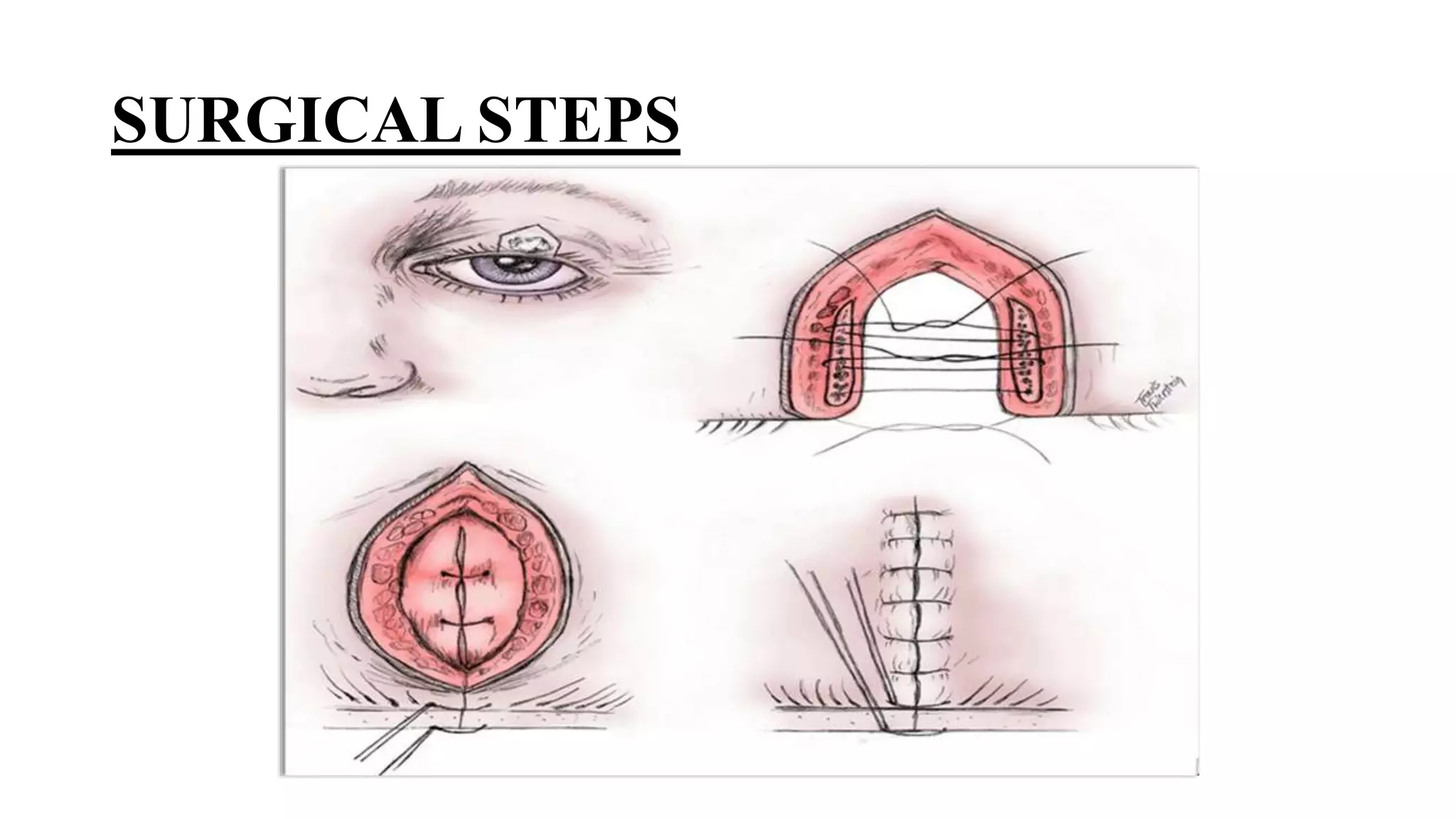
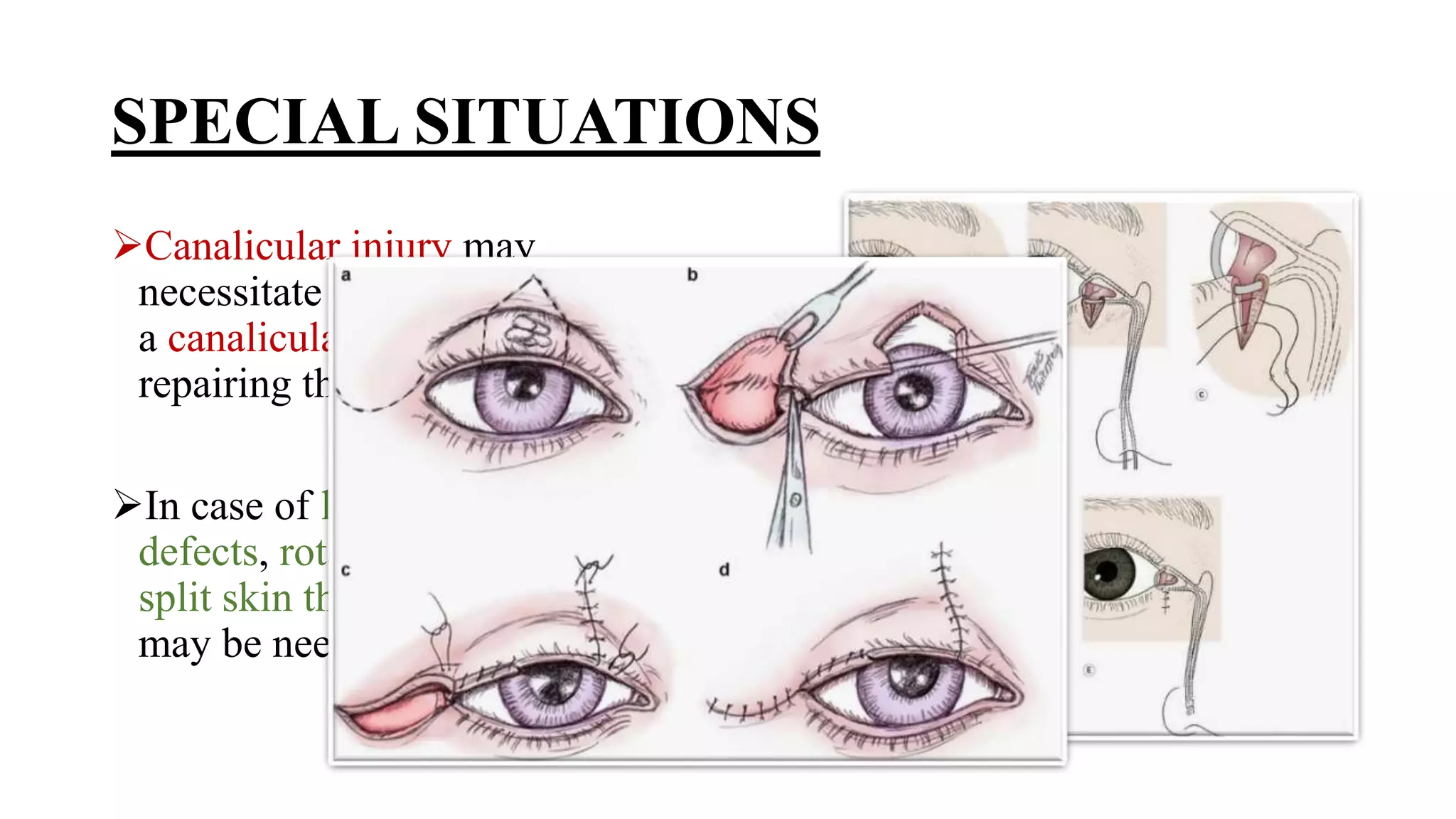
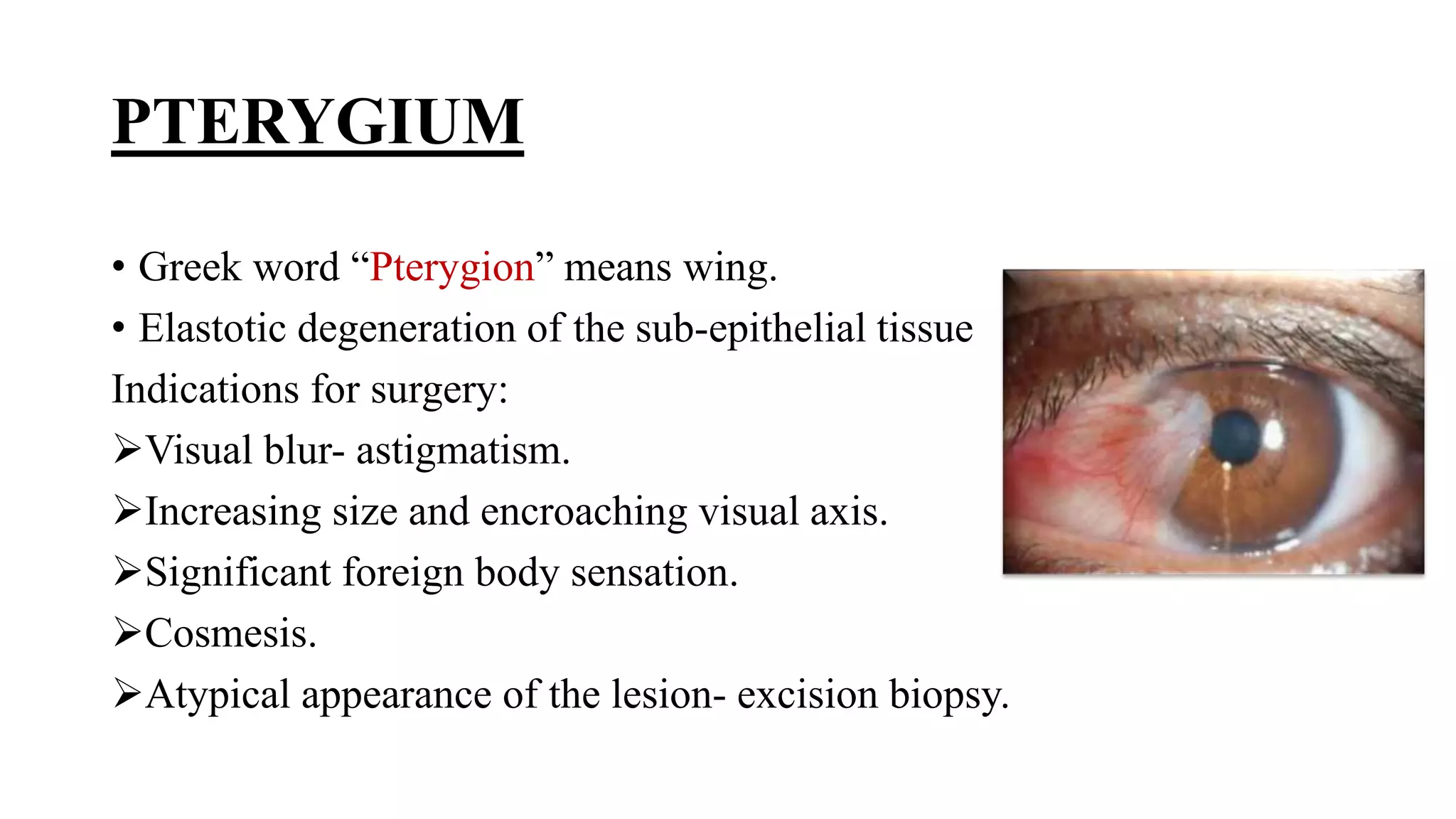
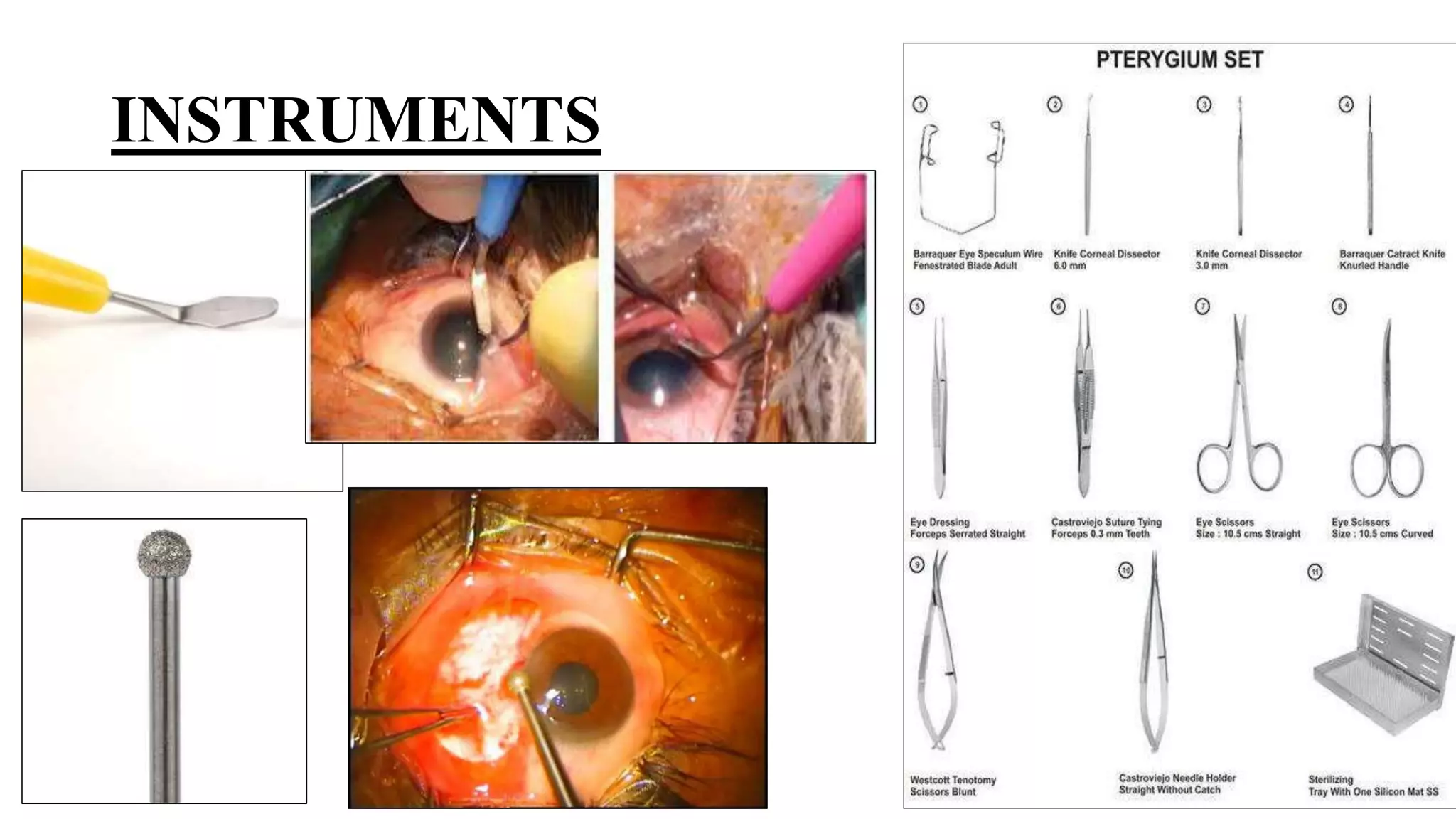
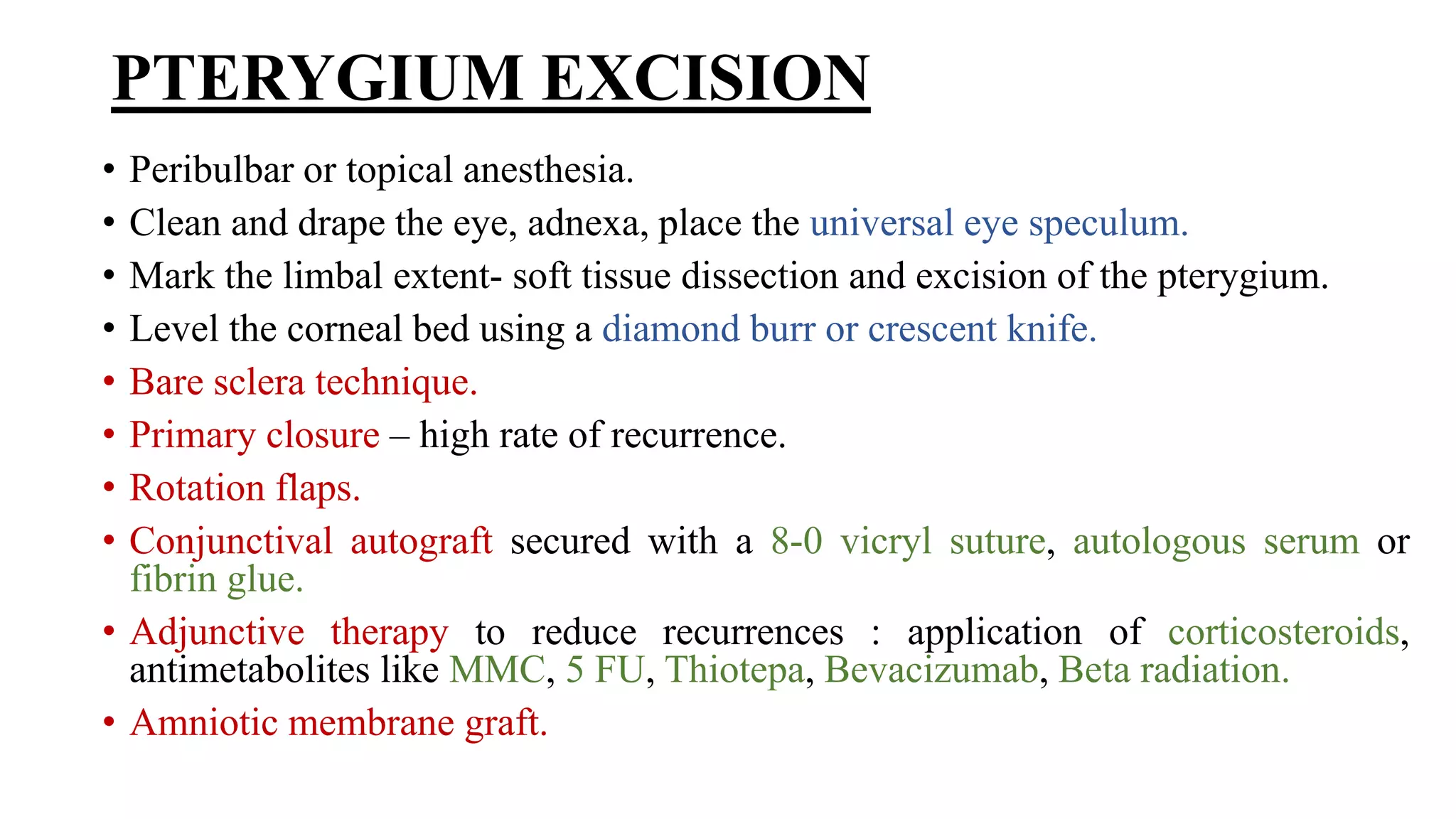
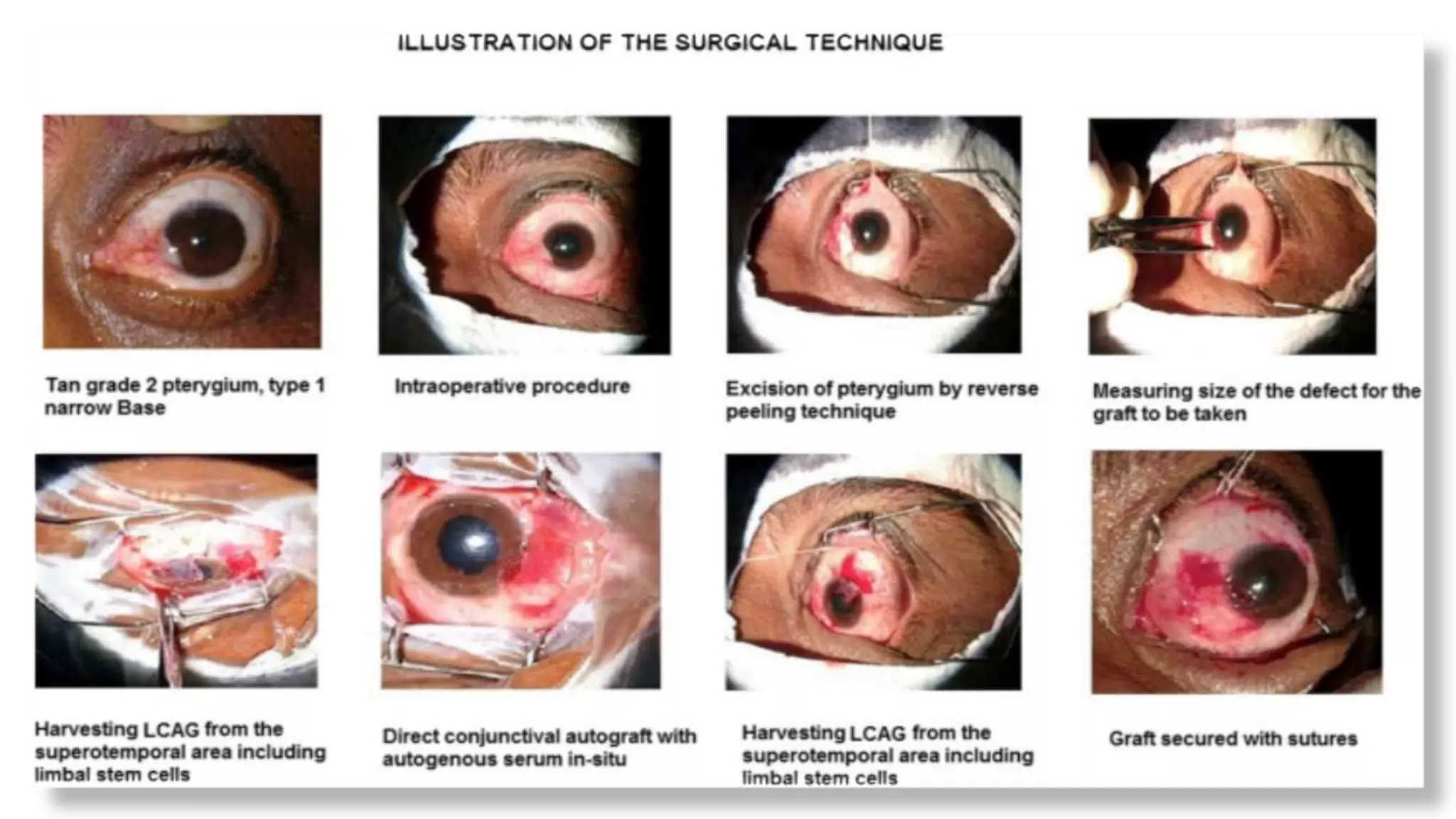
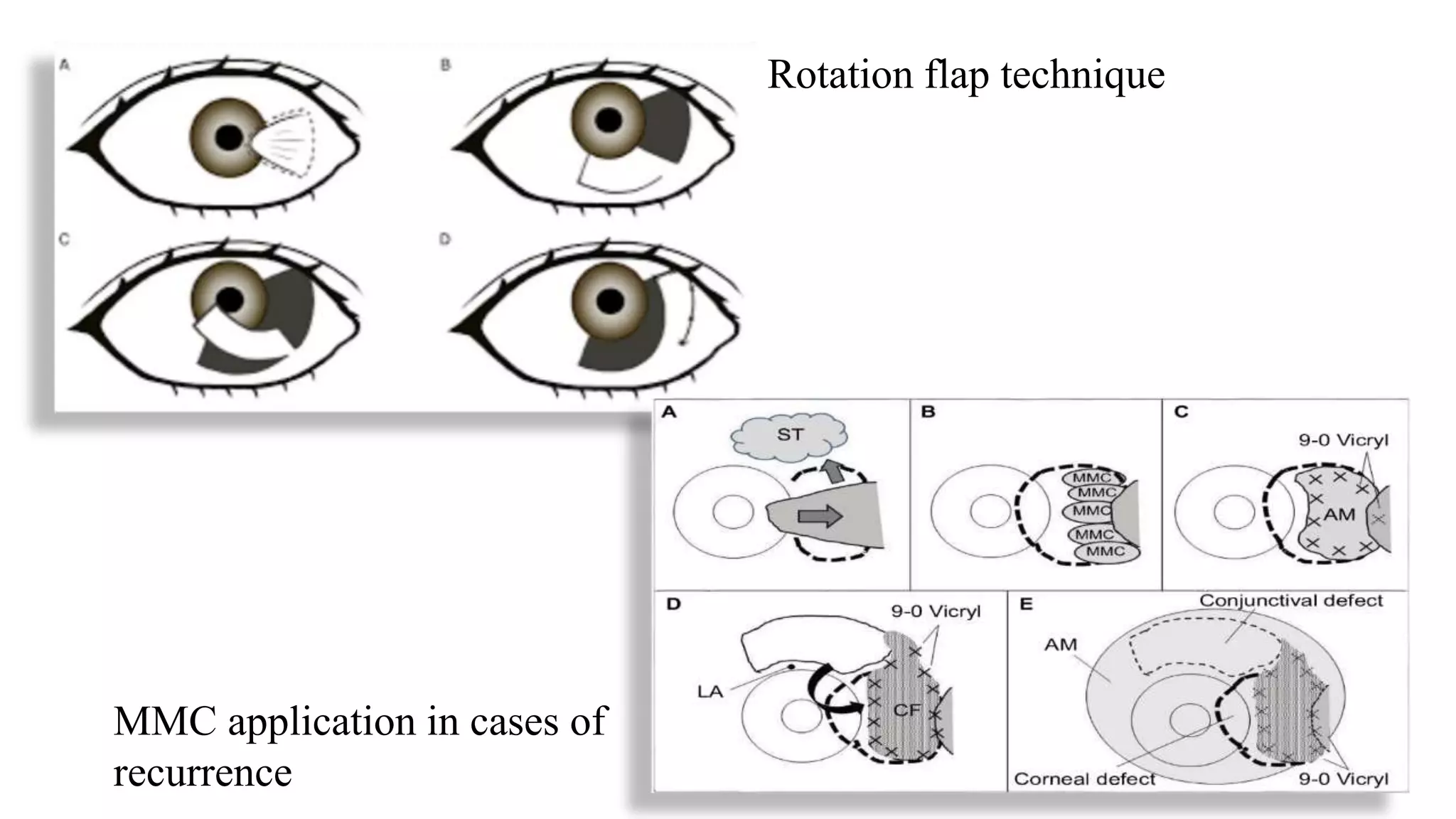
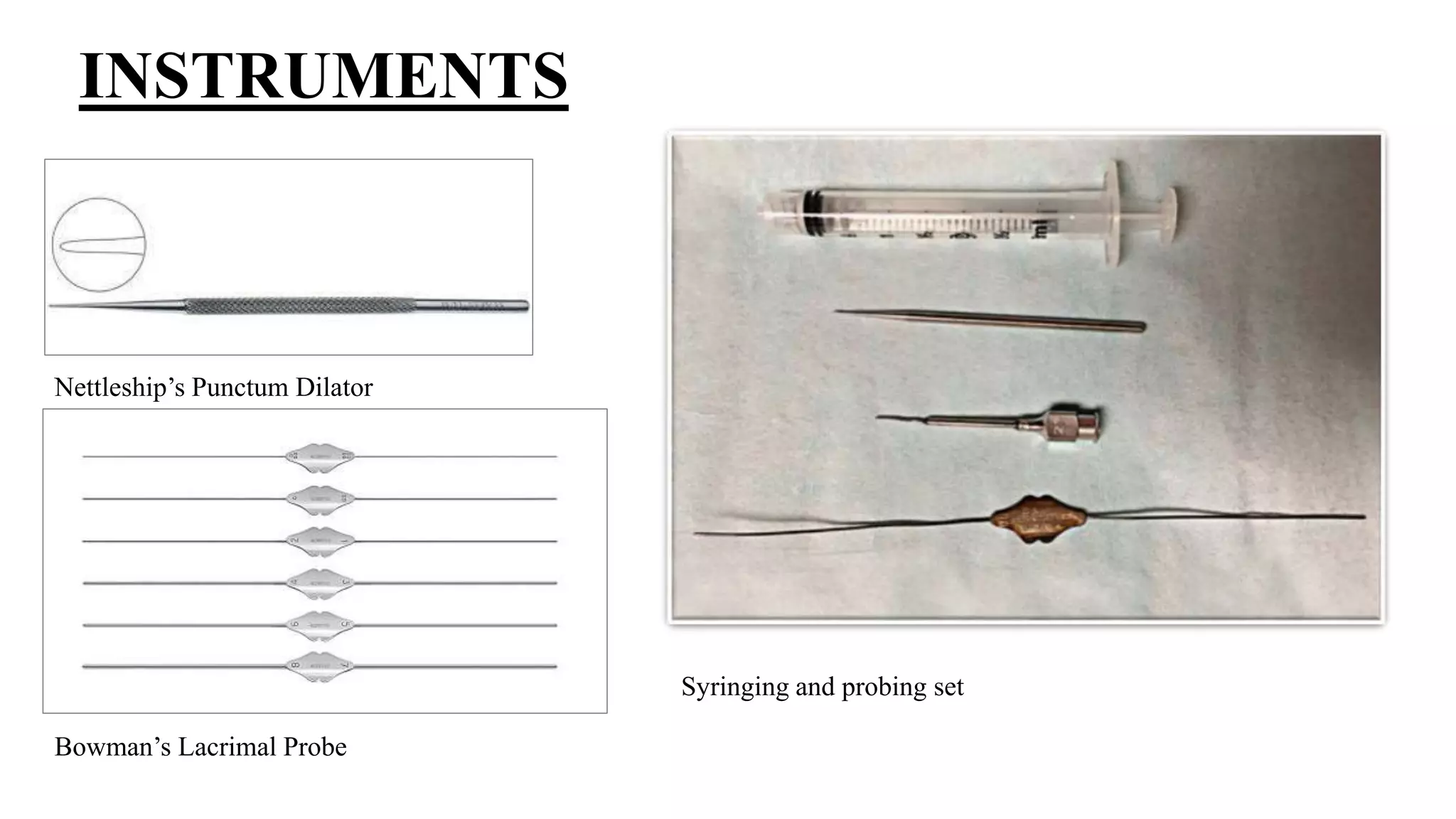
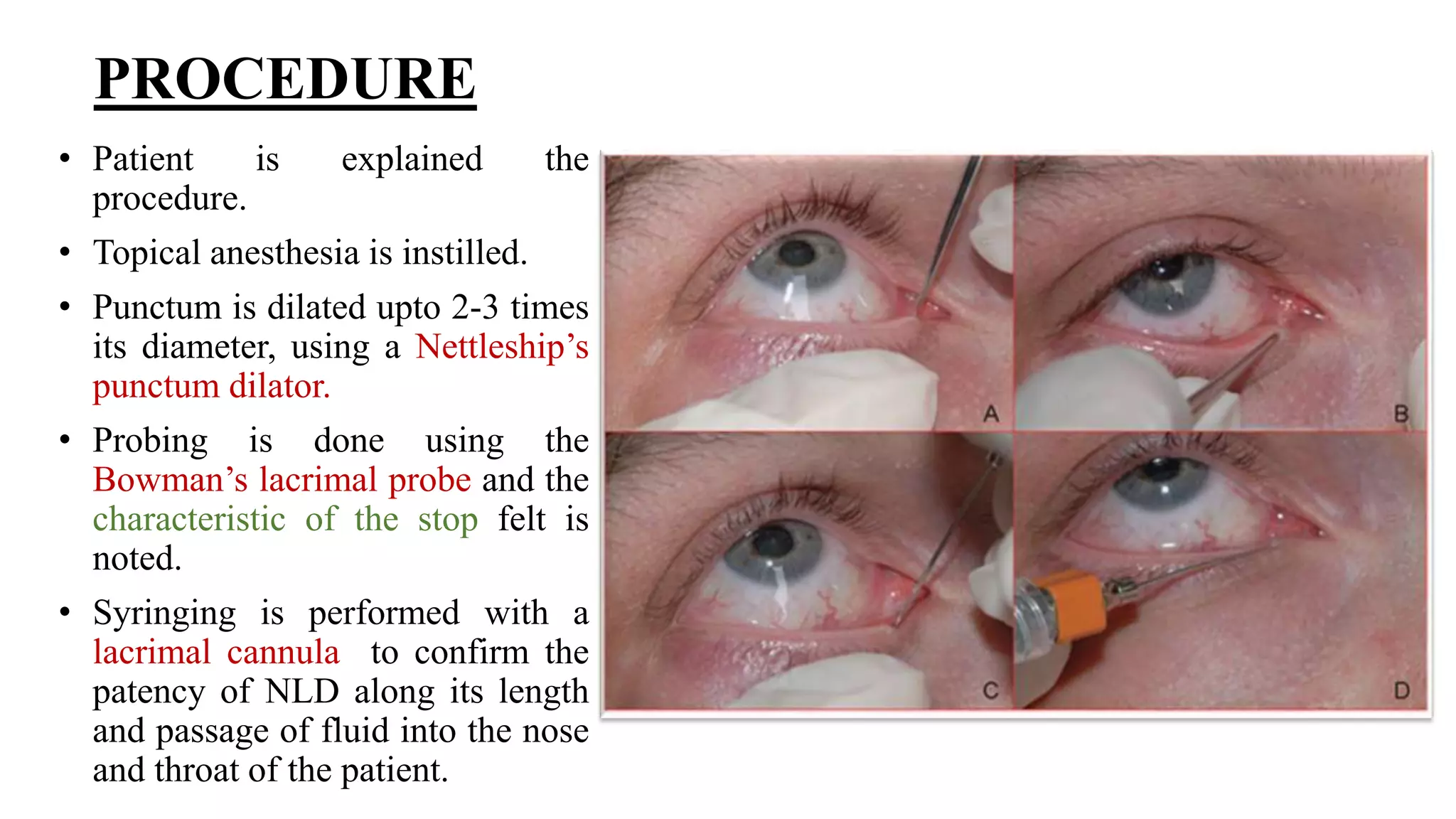
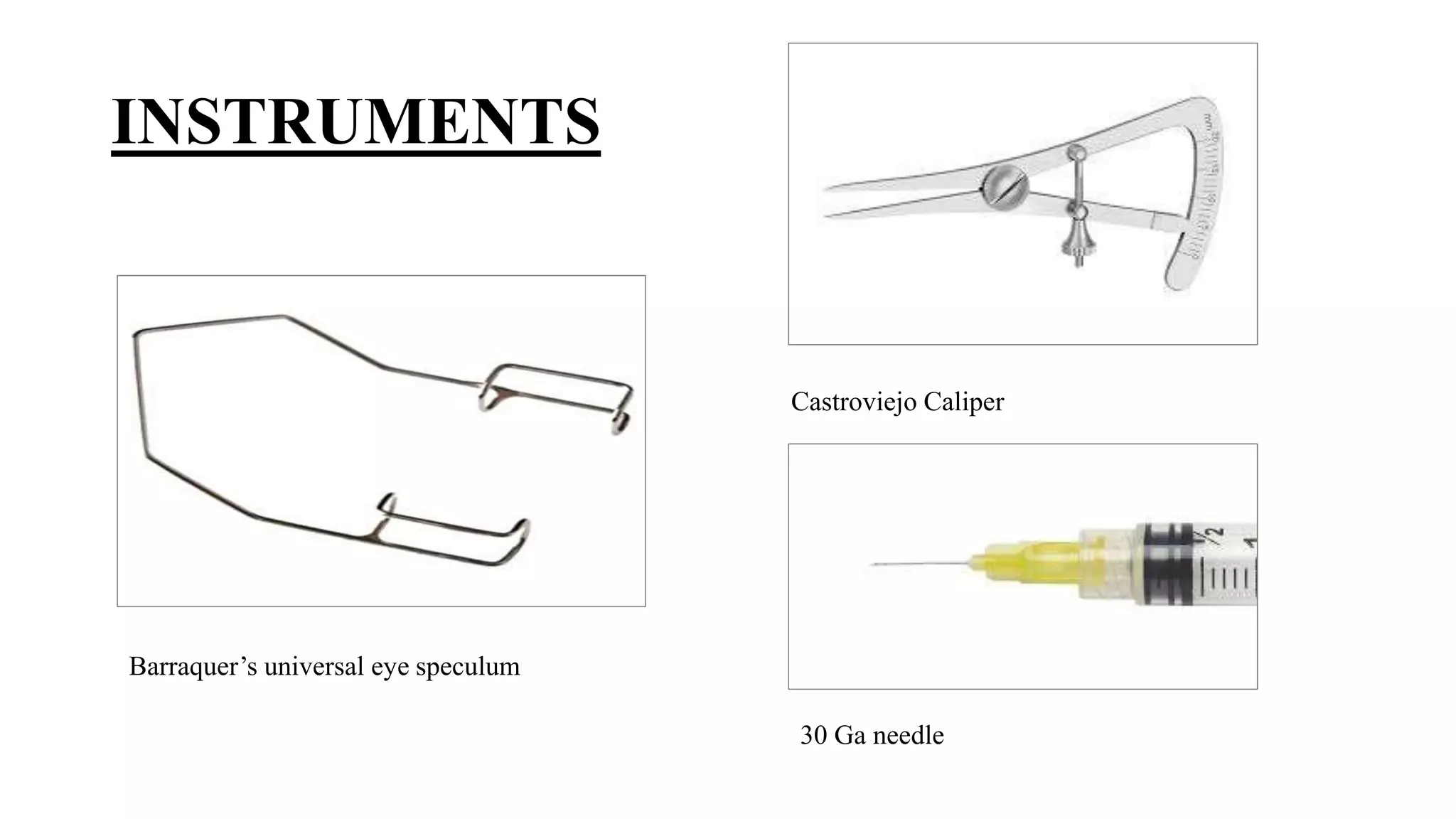
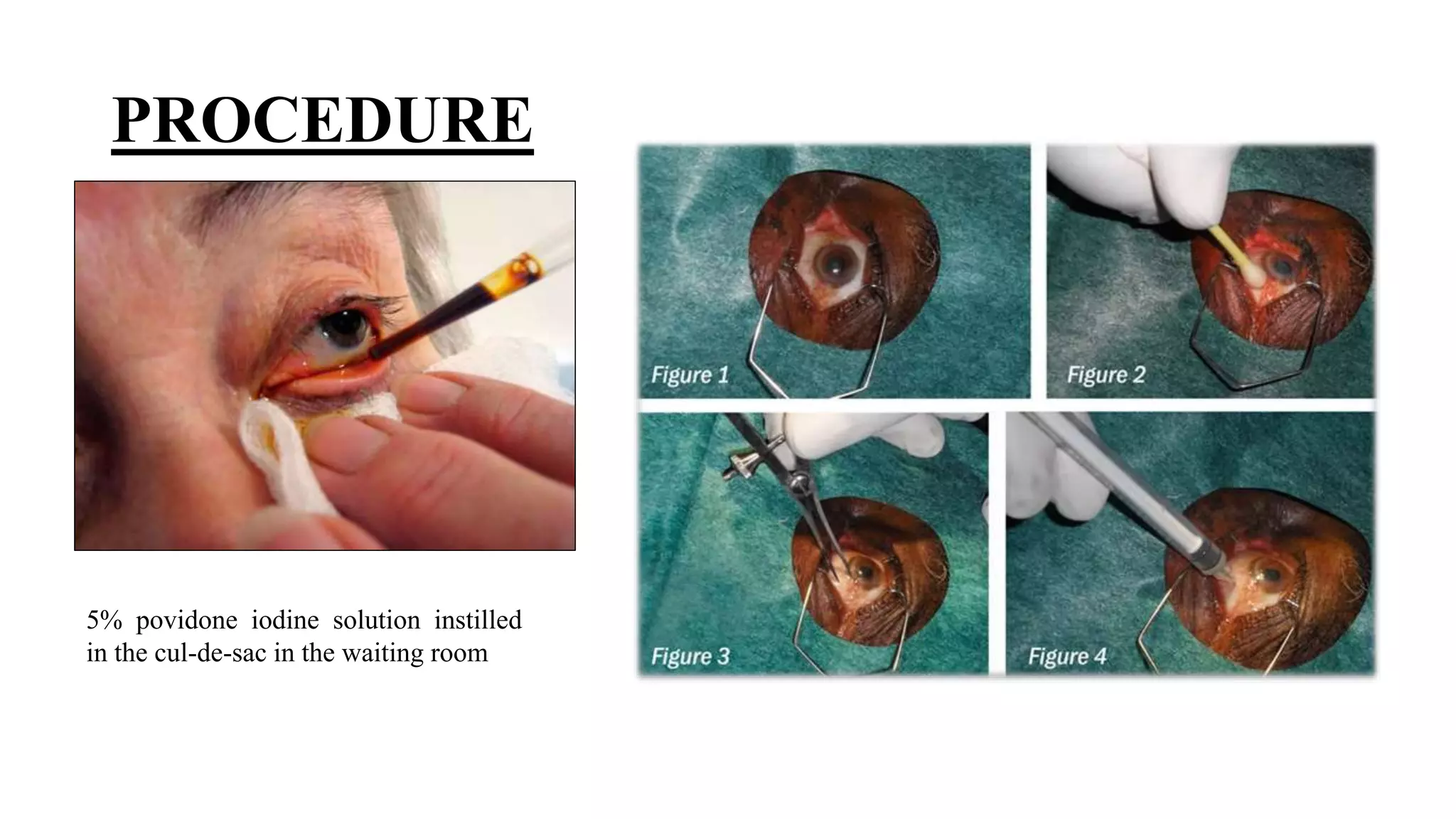

This document provides information on several minor ocular procedures including ocular irrigation, trichiatic eyelash removal, corneal foreign body removal, conjunctival suturing, suture removal, chalazion incision and curettage, lid laceration repair, pterygium excision, lacrimal probing and syringing, and intravitreal injections. It describes the indications, instruments, and steps for each procedure.











































![EYE REMOVAL TECHNIQUES [FINAL COPY BY FAITH KIMELI.] (1).pptx](https://cdn.slidesharecdn.com/ss_thumbnails/eyeremovaltechniquesfinalcopybyfaithkimeli-250203210808-e559c479-thumbnail.jpg?width=640&height=640&fit=bounds)






















