

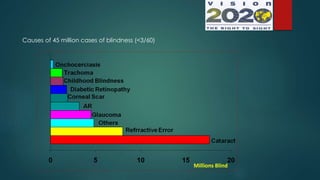
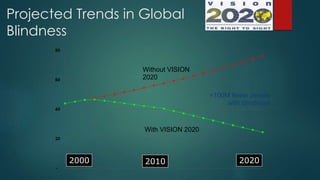
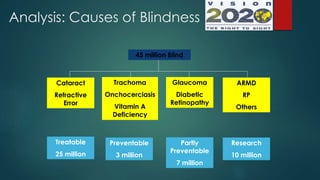












The document outlines Vision 2020, a global initiative to eliminate avoidable blindness. It notes that 80% of blindness is avoidable and without interventions, blind cases could rise to 75 million by 2020. Vision 2020's goal is to reduce blindness by 100 million cases worldwide by 2020 through prevention, treatment and rehabilitation. In India, Vision 2020 aims to eliminate avoidable blindness through strategies like strengthening eye care infrastructure, reducing major causes of blindness like cataract and childhood blindness, and developing human resources like training more eye care professionals. The key approaches involve implementing programs targeting major blinding conditions, developing a district-level eye care service model, and using appropriate technology.











































































































