Dacrocystectomy And Dacryocystorhinostomy presentation
1.
DEPARTMENT OF SHALAKYATANTRA
TOPICNAME : DACROCYSTECTOMY &
DACROCYSTORHINOSTOMY
PRESENTED BY : ANIL PAWAR
GUIDED BY : DR TUNDALWAR SIR
(HOD, DEPARTMENT OF SHALAKYATANTRA)
2.
DACROCYSTITIS
It isInflammation of Lacrimal Sac
Majorly Of Two types
1. Acute
2. Chronic
3.
It is thechronic suppurative inflammation of lacrimal sac
due to obstruction in the naso-lacrimal duct.
CHRONIC DACROCYSTITIS
4.
ETIOLOGY
A. Predisposing factors
1. Age - It is more common between 40 and 60 years of age.
2. Sex - The disease is predominantly seen in females (80%) probably due
to comparatively narrow lumen of the bony canal.
3. Race - It is rarer among Negroes than in Whites: as in the former NLD
is shorter, wider and less sinuous
4. Heredity - It plays an indirect role. It affects the facial configuration and
so also the length and width of the borsy canal.
5. Socio-economic status - It is more common in low socio-economic
group.6. Poor personal hygiene is also an important predisposing factor
5.
B. Factors responsiblefor stasis of tears in lacrimal sac
1. Anatomical factors, which retard drainage of tears include:
comparatively narrow bony canal, partial canalization of
membranous NLD and excessive membranous folds in NLD.
2. Foreign bodies in the sac may block opening of NLD.
3. Excessive lacrimation, primary or reflex, causes stagnation of
tears in the sac.
4. Mild grade inflammation of lacrimal sac due to associated
recurrent conjunctivitis may block the NLD by epithelial debris and
mucus plugs. It is the commonest one.
5. Obstruction of lower end of the NLD by nasal diseases such as
polyps, hypertrophied inferior concha, marked degree of deviated
nasal septum, tumours and atrophic rhinitis causing stenosis may
also cause stagnation of tears in the lacrimal sac.
6.
C. Source ofinfection –
Lacrimal sac may get infected from the conjunctiva, nasal
cavity (retrograde spread), or paranasal sinuses.
D. Causative organisms –
These include: Staphylococci, Pneumococci, Streptococci and
Pseudomonas pyocyanea.
Rarely chronic granulomatous infections like tuberculosis,
syphilis, leprosy and occasionally chinosporidiosis may also
cause dacryocystitis
7.
CLINICAL FEATURES
1.Stage ofchronic catarrhal
dacryocystitis:
It is characterised by mild
inflammation of the lacrimal sac
associated with blockage of NLD.
Watering eye is the only symptom
in this stage and sometimes mild
redness in the inner canthus.
On syringing the lacrimal sac,
either clear fluid or few mucoid
flakes regurgitate.
Dacryocystography reveals block
in NLD, a normal-sized lacrimal
sac with healthy mucosa.
2. Stage of lacrimal macocele :
It follows chronic stagnation causing
distension of lacrimal sac.
Characteristic features include
constant epiphora associated with a
swelling just below the inner canthus.
Regurgitation test. Milky or gelatinous
mucoid fluid regurgitates from the
lower punctum on pressing the
swelling.
Dacryocystography at this stage
reveals a distended sac with blockage
somewhere in the NLD.
Encysted mucocele.
8.
3. Stage ofchronic supporative
dacryocystitis.
Due to pyogenic infection, the
mucoid discharge becomes
purulent, converting the mucocele
into 'pyocoele.
The condition is characterised by
epiphora, associated recurrent
conjunctivitis and swelling at the
inner canthus with mild erythema
of the overlying skin.
On regurgitation a frank purulent
discharge flows from the lower
punctum.
If openings of canaliculi are
blocked at this stage the so called
4. Stage of chronic fibrotic sac.
Low-grade repeated
infections for a prolonged
period ultimately result in a
small fibrotic sac due to
thickening of mucosa, which
is often associated with
persistent epiphora and
discharge.
Dacryocystography, at this
stage reveals a very small sac
with mucosa
9.
MANAGEMENT
Medical treatment:Repeated sac syringing with
antibiotie-drops may clear the debris obstructing the
naso-lacrimal duct in the initial Stage only
Surgical treatment: If the condition is no cured by the
medical line of treatment then Dacryocystectomy or
Dacryocystorhinostomy should be performed.
ETIOLOGY
Acute dacryocystitis maydevelop in two ways:
1. As an acute exacerbation of chronic dacryocystitis.
2. As an acute peridacryocystitis due to direct involvement from the
neighbouring infected structures such as: paranasal sinuses,
surrounding bones and dental abscess or caries teeth in the upper
jaw.
Causative organisms Commonly involved are Streptococcus,
haemolyticus, Pneumococcus and Staphylococcus.
12.
CLINICAL FEATURES
Severepain and hot sensation over sac area.
Marked swelling with tenderness and redness of skin
is seen on the sac area
No regurgitation due to blocking of canaliculi due to
Oedema.
Slight conjunctival congestion.
Enlarged sub maxillary lymph node.
Fluctuation can be elicited if abscess is formed.
Lacrimal fistula due to repeated attacks.
13.
MANAGEMENT
Hot compress,local and systemic antibiotic, systemic analgesic and anti
inflammatory.
For Lacrimal abscess- a vertical incision is given for drainage of the pus.
Dacryocystectomy (DCT)-should be done after the inflammation is
controlled by medical treatment.
After single attack of acute Dacryocystitis, the sac shrinks and becomes
fibrous and hence dacryocystorhinostomy can not be performed
except in young adults with spontaneous attack i.e. without previous
history.
In lacrimal fistula complete excision of fistulous tract alongwith
excision of the sac should be done.
14.
DCT (DACRYOCYSTECTOMY)
Defination:It is a surgical procedure to remove the lacrimal sac.
Indications:
Elderly persons
1. After single attack of Acute Dacryocystitis (dacryocysto-
rhinostomy can not be performed due to fibrosis of sac wall)
Complications : Life Long Epiphora Due to removal of sac
15.
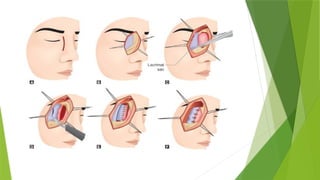
PROCEDURE
The sacarese is infiltrated with 2% Xylocaine with adrenaline for
local anesthesia (adrenaline should not be used in hypertensive
patient)
A curved 6mm incision is given 3mm to the nasal side of inner
canthus. The incision should be 2mm above medial palpebral
ligament
After splitting the orbicularis oculi muscle, Muller’s sac retractor is
applied preserving haemorrhage may occur.
Blunt dissection is performed till the sac is visible.
Sac is then separated up to the junction of naso lacrimal duct and
excised there.
Lacrimal fossa is cleaned and cauterized and the wound is
sutured preferably with continuous subcuticular Sutures for
Cosmetic purpose
17.
DCR (DACRYO-CYSTO-RHINOSTOMY)
Defination:It is a nasal drainage operation in which there is no
epiphora post-operatively if the operation is successful
Indications : Young patient with Chronic dacrocystitis
Complications:
Hemorrhage either from angular vein or from nasal mucosa (hence
pack should not be removed before 24 hours).
1. Failed DCR- small opening in the lacrimal bone, fragile mucous
membrane due to old age and post operative infection.
18.
PROCEDURE
The nasalcavity of the same side is packed with a ribbon gauge soaked
in 4% xylocaine.
All the steps up to the exposure of the sac are same as
dacryocystectomy.
The lacrimal bone is exposed by incising periosteum over the lacrimal
crest.
Bone is removed with a gauge and hammer or bone punch so that the
nasal mucosa is exposed.
A vertical incision is made on the sac and the mucous membrane and
their walls are anastomosed. The wound is cleaned and dressed as
before.
Syringing is done on the first post operative day to test the patency of
the passage
Post-op Analgesics and anti-biotic should be given