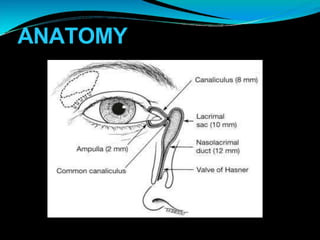
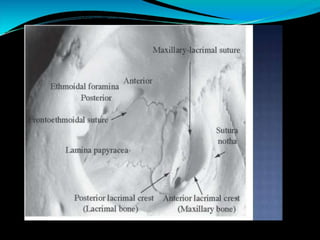
This document describes the surgical procedure for lacrimal sac surgery. It details the indications, preoperative requirements, steps of the surgery including nasal packing, skin incision, exposure of the maxillary punctum and lacrimal crest, bone removal, preparation and suturing of sac flaps, reattachment of tissues, and post-operative care. The goal of the surgery is to create a drainage pathway between the lacrimal sac and nasal cavity for tears when previous treatments for blockages have failed. Adjunctive measures like mitomycin C or intubation may be used for complex cases.