Downloaded 579 times




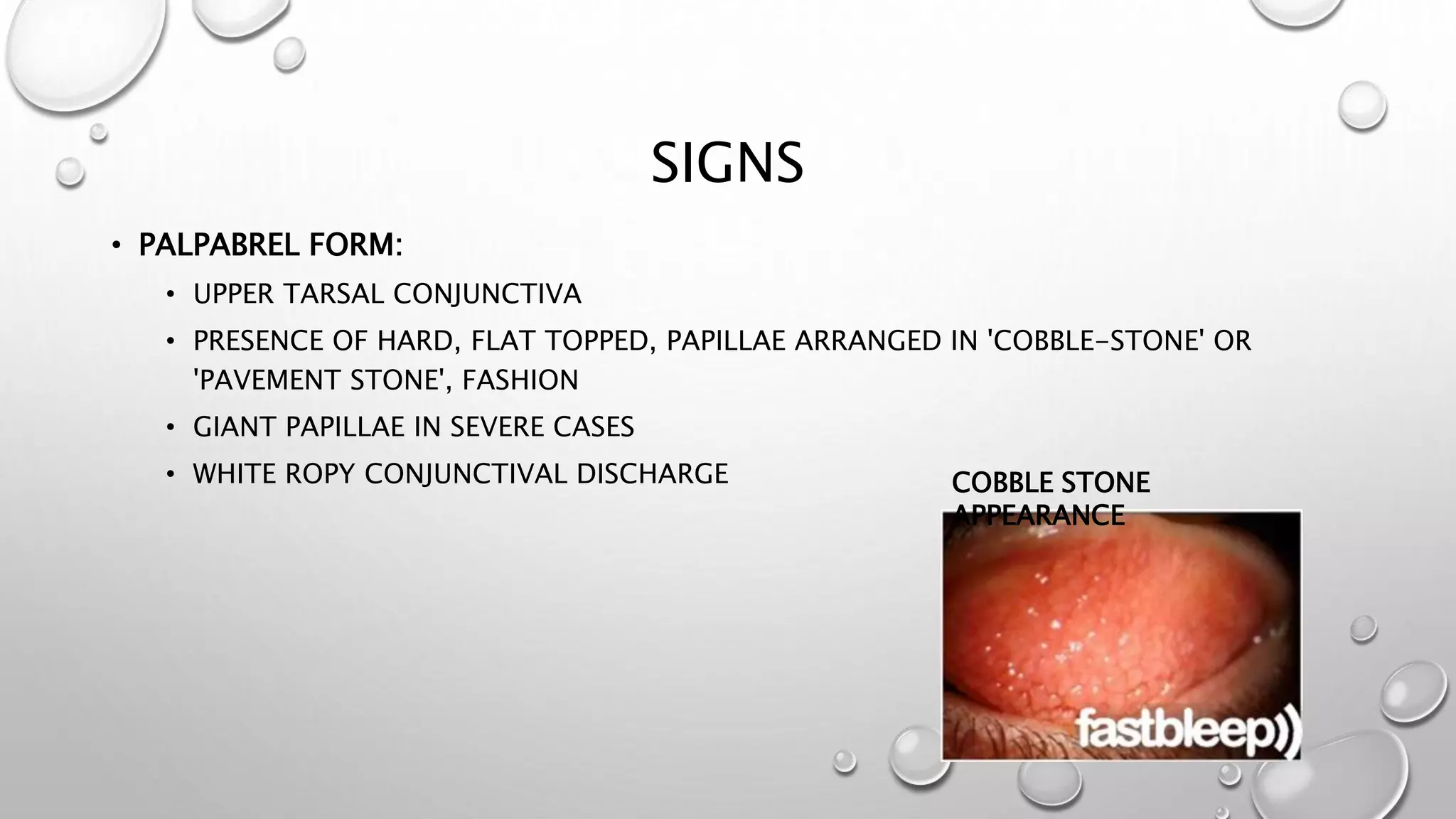
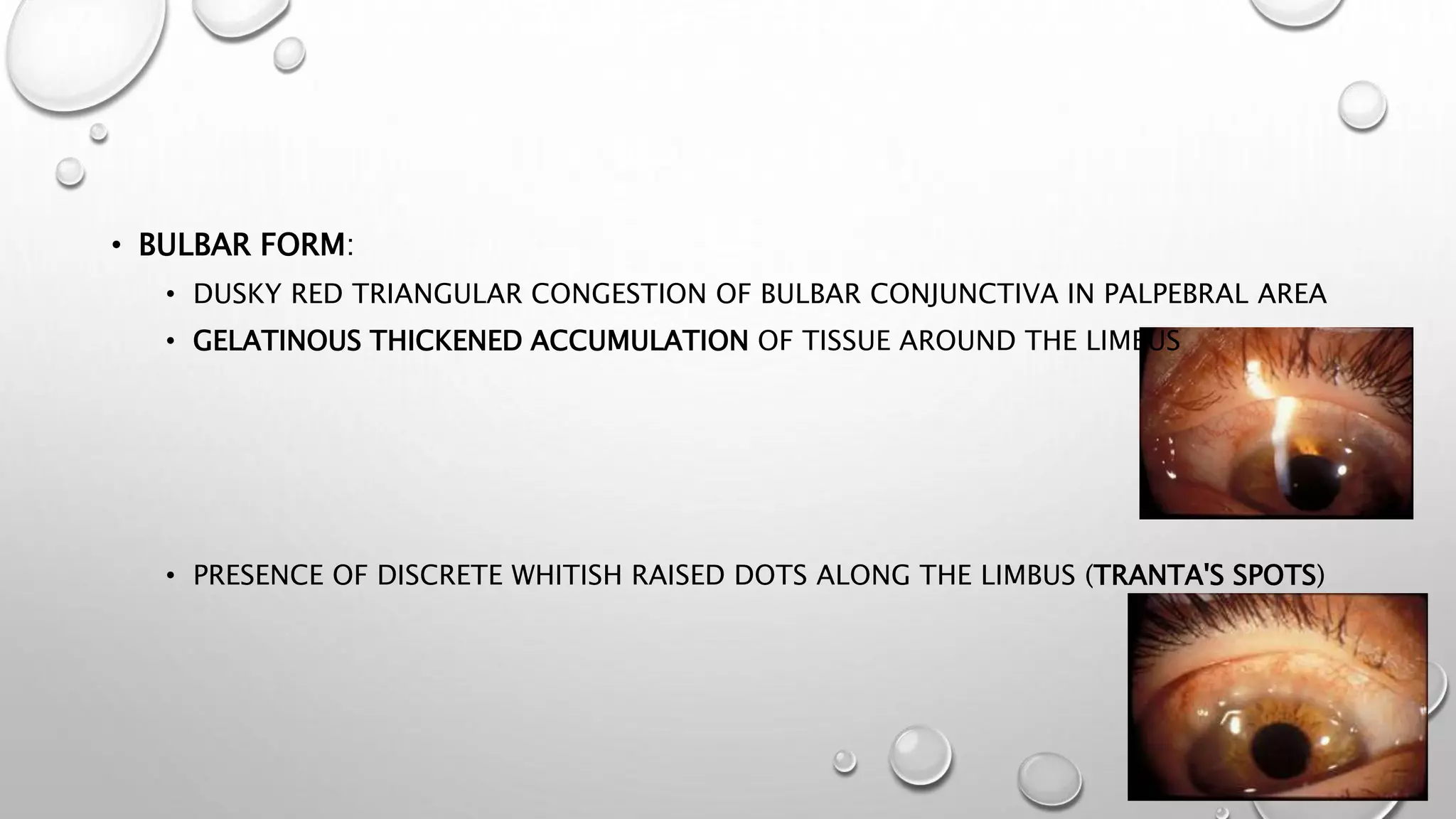


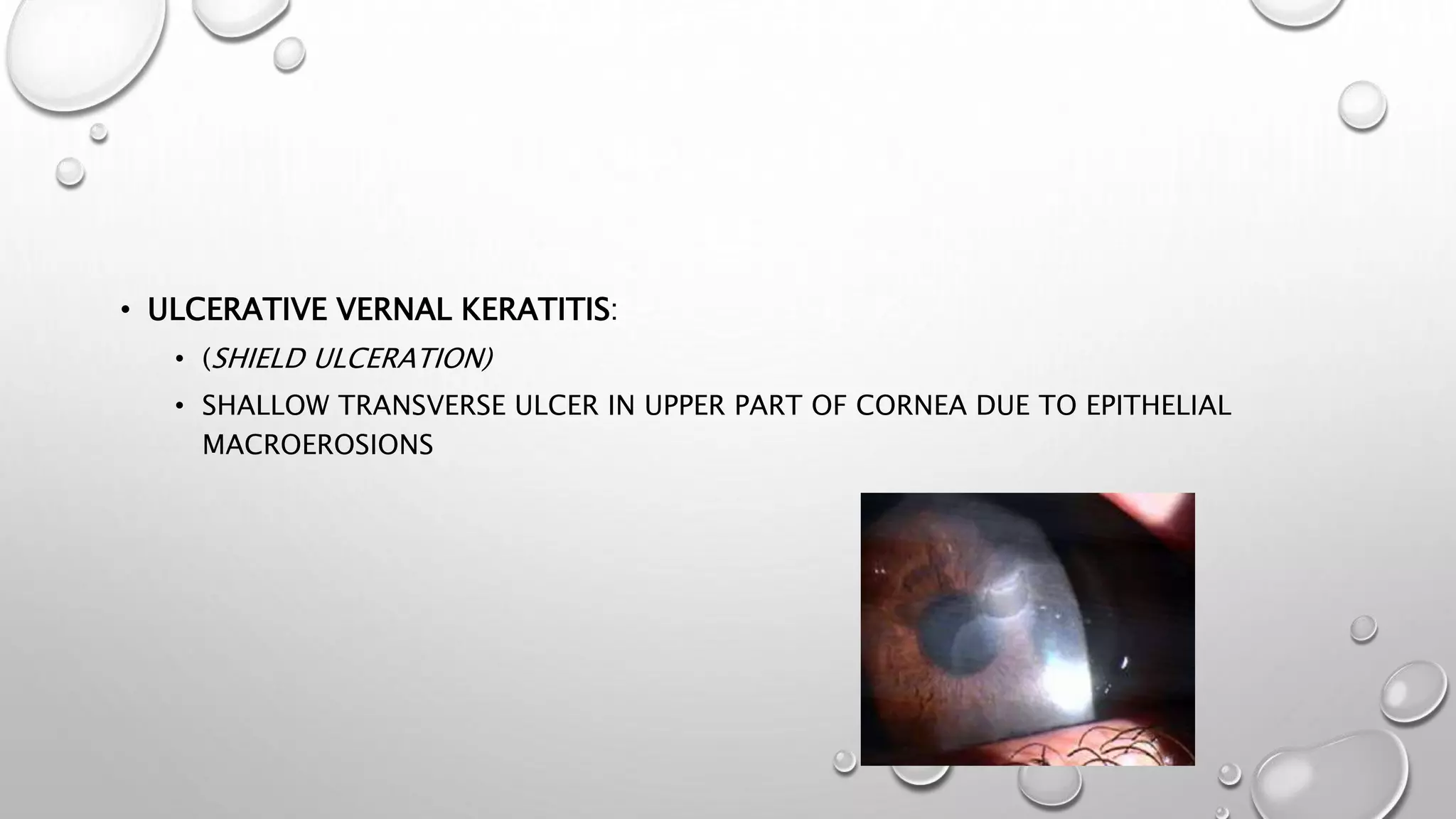

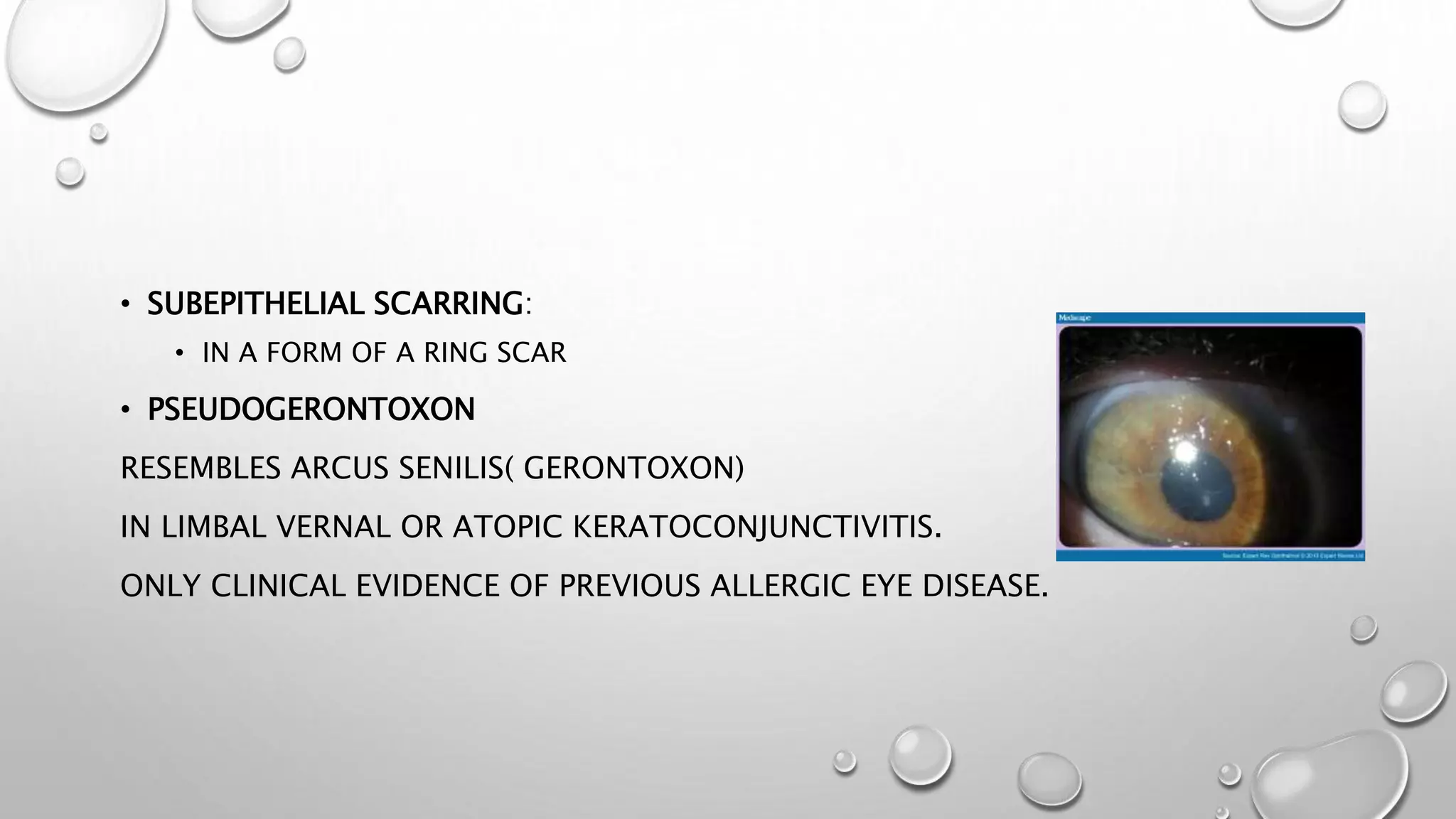







This document discusses vernal keratoconjunctivitis (VKC), a recurrent, seasonal eye condition seen primarily in children and young adults. VKC involves inflammation of the conjunctiva and cornea and is caused by an allergic reaction, often to pollen allergens. Symptoms include itching, tearing, and thick discharge. Signs include raised papillae on the conjunctiva that resemble cobblestones. Treatment focuses on reducing inflammation and symptoms using topical steroids, mast cell stabilizers, and antihistamines. The condition typically resolves spontaneously by adulthood.



































































































