




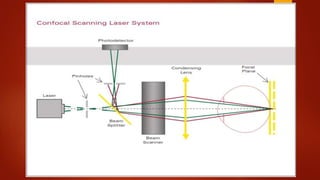





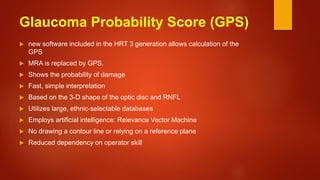
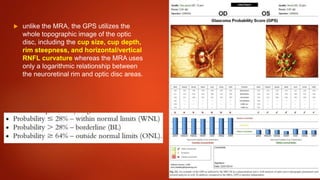



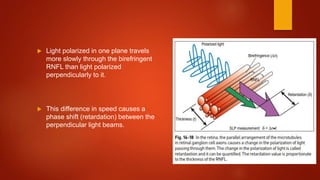
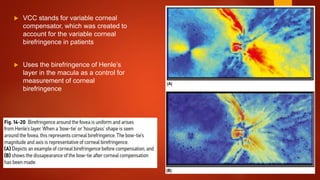
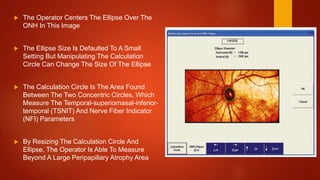
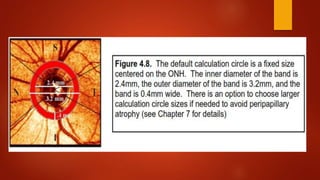


The document discusses two imaging techniques used to detect glaucoma - HRT (Heidelberg Retinal Tomography) and GDx (scanning laser polarimetry). HRT uses confocal scanning laser ophthalmoscopy to generate a 3D topographic image of the optic disc and retinal nerve fiber layer. GDx measures the retinal nerve fiber layer thickness around the optic disc using scanning laser polarimetry, which analyzes the polarization of light passing through the birefringent retinal nerve fiber layer. Both provide objective measures of the optic disc and retinal nerve fiber layer but have limitations such as dependency on accurate contour line placement for HRT.












![Types of pediatric contact lens [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/typesofpediatriccontactlensautosaved-200210123904-thumbnail.jpg?width=640&height=640&fit=bounds)



























































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


