Visual evoked potential
•Download as PPTX, PDF•
175 likes•39,381 views

The document discusses visual evoked potentials (VEPs), which involve recording electrical signals from the visual cortex in response to visual stimulation. It notes that VEPs have smaller amplitudes than EEGs but can objectively assess macular function and the functional state of the visual system. It describes how steady state VEPs use rapid stimulation to produce sinusoidal waveforms while transient VEPs use discrete deflections with low rates of stimulation. It also discusses the use of flash VEPs, pattern VEPs, and other techniques and provides details on stimulation methods, components of VEP testing equipment, factors that influence VEPs, and abnormal findings that may be observed in various conditions.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Visual evoked potential
Similar to Visual evoked potential (20)
More from SSSIHMS-PG
More from SSSIHMS-PG (20)
Visual evoked potential
- 2. • Record of gross electrical signal generated at visual (occipital) cortex in response to visual stimulation • The amplitude of VEP-3 to 25 microvolt is considerably smaller than that of EEG, which can be as large as 100 microvolt
- 3. • Averaged and amplified record of action potentials in visual cortex • VEP is the only objective technique available to assess clinically the functional state of the visual system beyond the retinal ganglion cells.
- 5. • Since foveal projection is magnified at cortex , it is an objective indication of macular function
- 6. • At rapid rates of stimulation the waveform becomes sinusoidal – STEADY STATE VEP • Not used routinely due to inferior information on latency • Low rates of stimulation – discrete deflections • Known as TRANSIENT VEP • This is commonly employed
- 8. • FLASH • Occipital cortex is relatively insensitive to flash • PATTERN • Cortex is sensitive to edges of contrast
- 11. • Response to diffusely flashing light stimulus that subtends a visual field of 20 degrees • Cruder response than pattern VEP • Merely indicates that light has been perceived by cortex • Indications – media haze, infants,poor patient cooperation
- 12. • Response to a patterned stimulus - checkerboard or square and sine wave gratings • Frequency of gratings is decribed in CPD- cycles per degree • For check pattern visual angle subtended by a single check is used • Preferred technique for most clinical purposes, gives an estimate of form sense and thus visual acuity
- 13. • A pattern is abruptly exchanged with an equilluminant diffuse background • More intersubject variability than pattern reversal VEP • Useful in detection of pts with malingering , pts with nystagmus
- 14. • There should be no distracting sound or light waves • Pattern and flash must both be done in all patients as pattern cannot be detected in pts with media opacities • Pattern VEP followed by flash VEP • Significantly affected by eccentric fixation, excessive blinking of eyes and partial closure of eyes
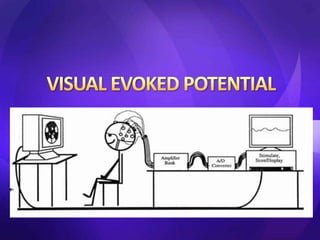
- 15. • Visual stimulus producing device • Scalp electrodes • Amplifier • Computer and read out systems
- 17. • Undilated pupil • Monocular recording • Refractive correction • Relaxed position • 1m distance from monitor
- 22. • P 100 LATENCY ( m sec ) = 102 5 • R-L difference ( msec) = 1.3 2.0 • Amplitude (μV) =10 4.2 • Duration = 63 8.7
- 23. • If acuity of the patient is in question , the amplitude is more important • If detection of a lesion in visual pathway is in question , latency is more important • Latency is more reliable than amplitude (Variabilty – 5% as compared to 25%)
- 24. • Presence of reduced amplitude is non specific, gains importance only on serial testing • B/L symmetry is seen both with flash and pattern VEP , thus an asymmetrical response is more indicative of an abnormality
- 25. • SIZE OF STIMULUS – Decrease in size of stimulus increases amplitude of VEP • Position of electrodes on scalp • AGE- amplitude decreases with age • ATTENTION OF PATIENT – If subject looks to side of stimulus , there is rapid fall in size of response
- 26. DELAYED LATENCY • Demyelinating optic neuritis • Neurotransmitter disorders • Glaucoma • Uncorrected refractive error • Ageing REDUCED AMPLITUDE • Optic atrophy • Toxic • Compressive • Uncorrected refractive error • Ambylopia
- 27. • OPTIC NEURITIS / MULTIPLE SCLEROSIS Increased latency of P100 Even when no defect in visual acuity , colour vision or field of vision. About 96% of pts with MS have delayed latency
- 28. • COMPRESSIVE OPTIC NERVE LESIONS – decreased amplitude without much change in latency • DURING ORBITAL OR NEUROSURGICAL PROCEDURES- continuous record of optic nerve function in form of VEP to prevent inadvertent damage to the nerve during surgical manipulation
- 29. • DEGENERATIVE DISEASES that affect the spinal cord, cerebellar pathways, or both, such as Friedreich's ataxia, Huntington's disease, neurosyphilis, and AIDS, also can affect the optic nerves and cause visual defects, including a delay of the pattern VEP
- 30. • The earliest VEP abnormalities in LEBER'S optic neuropathy appear to be increases in P100 latency or changes in the waveform morphology (i.e., the development a double positive peak). • As the condition progresses, the VEP amplitude decreases to a point where responses become immeasurable.
- 31. • Patients with THYROID OPHTHALMOPATHY may have a prolonged latency of the pattern VEP before a clinically apparent optic neuropathy.55 • SUBACUTE COMBINED DEGENERATION secondary to vitamin B12 deficiency causes demyelination and prolongs the pattern VEP latency,56,57 even with an unremarkable neuroophthalmologic examination.58
- 32. • AION Low amplitude but normal latency TO ASSESS MISPROJECTION OF OPTIC NERVE FIBRES IN ALBINISM Nerve fibers that originate in the temporal retina are misrouted at the optic chiasm. This misrouting results in an anomalous temporal nerve fiber decussation and an abnormal projection to the occipital cortex.-definite VEP asymmetry
- 33. • TO ASSESS VISUAL POTENTIAL IN PATIENTS WITH OPAQUE MEDIA • Flash VEPs may be useful for detecting maculopathy or optic neuropathy in patients with dense media opacities. • An amplitude reduction of more than 50% or a latency delay of more than 15 ms is highly suggestive of dysfunction in the central visual field. • important in patients with opacities who are at high risk for neuronal dysfunction, such as patients with diabetes, ocular hypertension, or ocular trauma.
- 34. • TO ASSESS VISUAL ACUITY IN NON VERBAL CHILDREN , MENTALLY CHALLENGED AND APHASIC PATIENTS • Useful in assessing the integrity of macula and visual pathway • Pattern VEP gives a rough estimate of visual acuity objectively
- 35. • EVALUATION OF OPTIC NERVE FUNCTION IN PATIENTS WITH HEAD INJURY • Pupillary reflexes are often inaccessible because of periocular edema and/or motoric pupillary involvement, and patients are often comatose or sedated. Under these circumstances, the flash VEP can provide valuable information regarding optic nerve integrity. AMBYLOPIA – decrease in amplitude with relative sparing of latency
- 36. • GLAUCOMA • Decreases in pattern VEP amplitude and prolonged VEP latencies are found in many patients with glaucoma and some glaucoma suspects • Steady-state VEPs appear to be more sensitive for detecting glaucomatous damage thantransient responses
- 37. • MALINGERING AND HYSTERICAL BLINDNESS • R/O malingering by confirming the fact that visual pathway is intact even in patients claiming no PL • Hysterical response – shows large variations from moment to moment , eg first half may produce an absent VEP and second half may produce normal VEP
- 38. • VISUAL FIELD DEFECTS • Asymmetry of amplitudes of VEP recorded over each hemisphere implies a hemianopic visual pattern • Decreased amplitude of VEP recorded over contralateral hemisphere when each eye is stimulated separately indicates bitemporal field defect
- 39. • Generated simultanously from 60 regions of central 20 to 25 degrees of visual field • Local defects are easily missed in conventional VEPS • Can detect local demylination - f/u of cases of optic neuritis • To confirm unreliable visual fields
- 40. THANK YOU