Downloaded 1,480 times

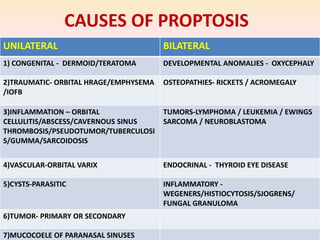










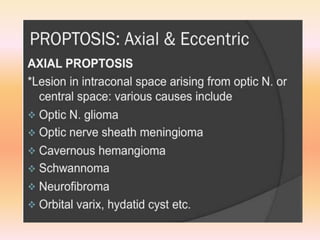
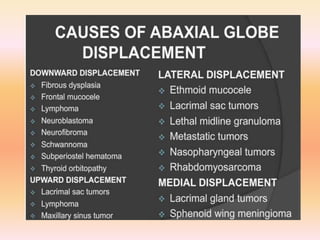



















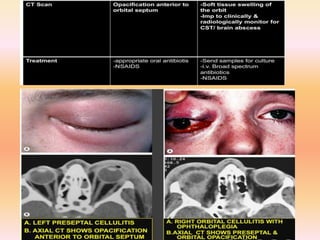





- The document discusses the evaluation of proptosis, which is the abnormal forward protrusion of the eyeball. It defines different types of orbital abnormalities and provides the approach to examining a patient with proptosis, including taking a thorough history, performing a local and systemic examination, ordering appropriate imaging and lab tests, and considering histopathological studies if needed. The causes of proptosis can be divided into categories such as inflammatory, mass effect, vascular changes, and infiltrative processes. Key aspects of the evaluation are to determine if the proptosis is unilateral or bilateral and whether there are associated signs and symptoms to suggest an underlying cause.



































































