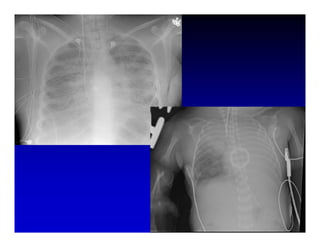
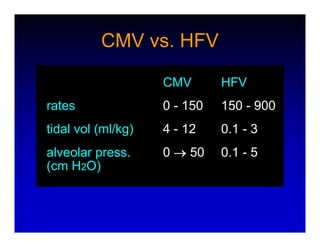

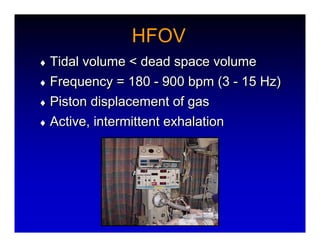
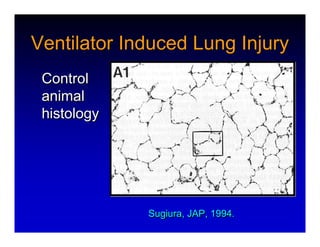
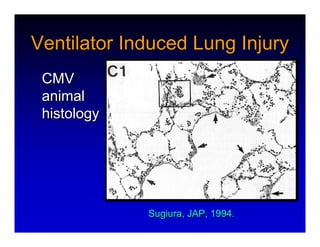
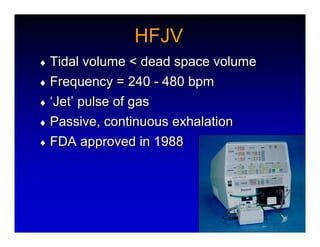

1. High frequency ventilation (HFV) uses small tidal volumes and high respiratory rates to ventilate patients with acute lung injury (ALI) or acute respiratory distress syndrome (ARDS). HFV aims to recruit and protect the injured lung better than conventional mechanical ventilation (CMV). 2. Two main types of HFV are high frequency oscillatory ventilation (HFOV) and high frequency jet ventilation (HFJV). HFOV uses a piston to displace gas at 180-900 breaths per minute, while HFJV uses gas jets at 240-480 bpm. 3. Early intervention with HFV may improve outcomes compared to using it as a rescue therapy after prolonged CMV fails. Matching the











































































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)